In the following table, we include the studies comparing AHSCT vs other DMTs. The table shows that none of the DMTs worked better clinically or radiologically than AHSCT.
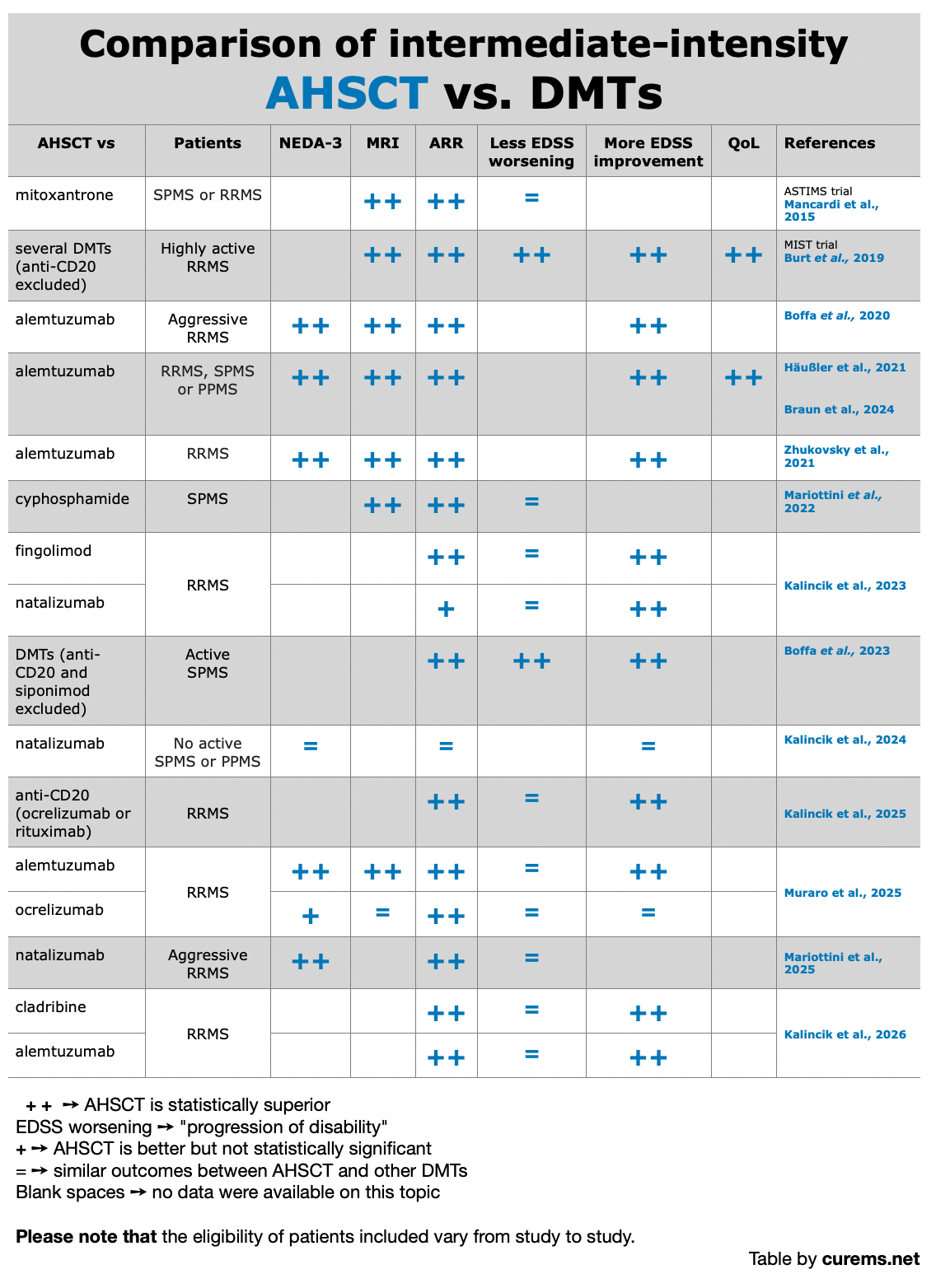
- NEDA-3 – No Evidence of Disease Activity: means no relapses, no new MRI lesions, and no worsening of disability.
- ARR – Annualized Relapse Rate: the average number of relapses a person has in one year.
- MRI – Magnetic Resonance Imaging: a brain scan that shows if there are new or active lesions related to MS.
- Less EDSS worsening – fewer people showed worsening of disability (based on the EDSS scale).
- More EDSS improvement – more people showed improvement in their level of disability (based on the EDSS scale).
- QoL – Quality of Life: how good and satisfying daily life feels, including physical, emotional, and social well-being.
Studies cited in the table above:
- Mancardi et al., 2015
- Burt et al., 2019
- Boffa et al., 2020
- Häubler et al., 2021 | Braun et al., 2024
- Zhukovsky et al., 2021
- Mariottini et al., 2022
- Kalincik et al., 2023
- Boffa et al., 2023
- Kalincik et al., 2024
- Kalincik et al., 2025
- Muraro et al., 2025
- Mariottini et al., 2025
- Kalincik et al., 2026
Clinical Studies
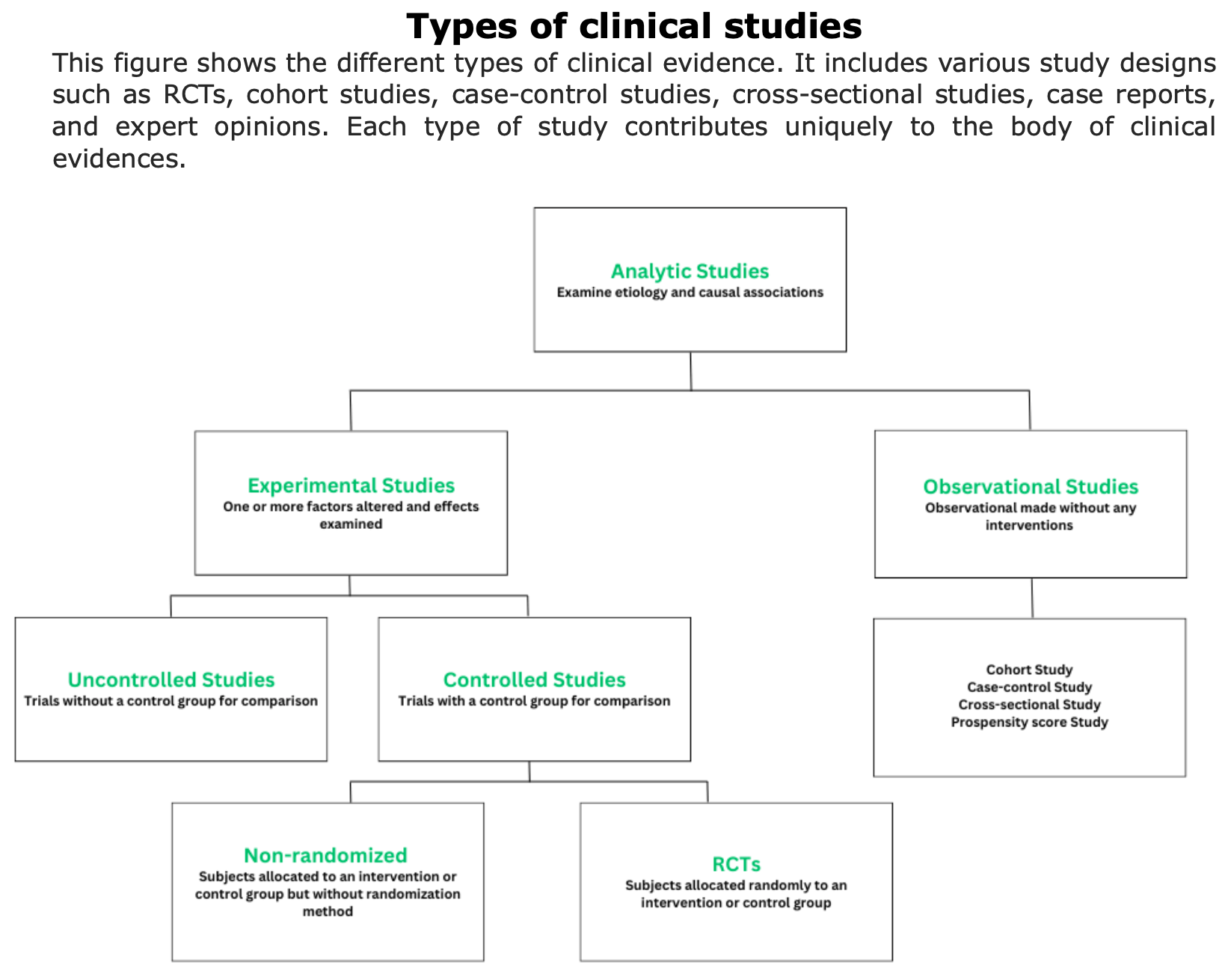
What kinds of studies are done to assess whether a treatment is effective?
There are different types of studies, each providing evidence of varying strength. CureMS.net adopts the study classification known as the “pyramid of evidence” (see figure below), which ranks studies according to the quality of their evidence.
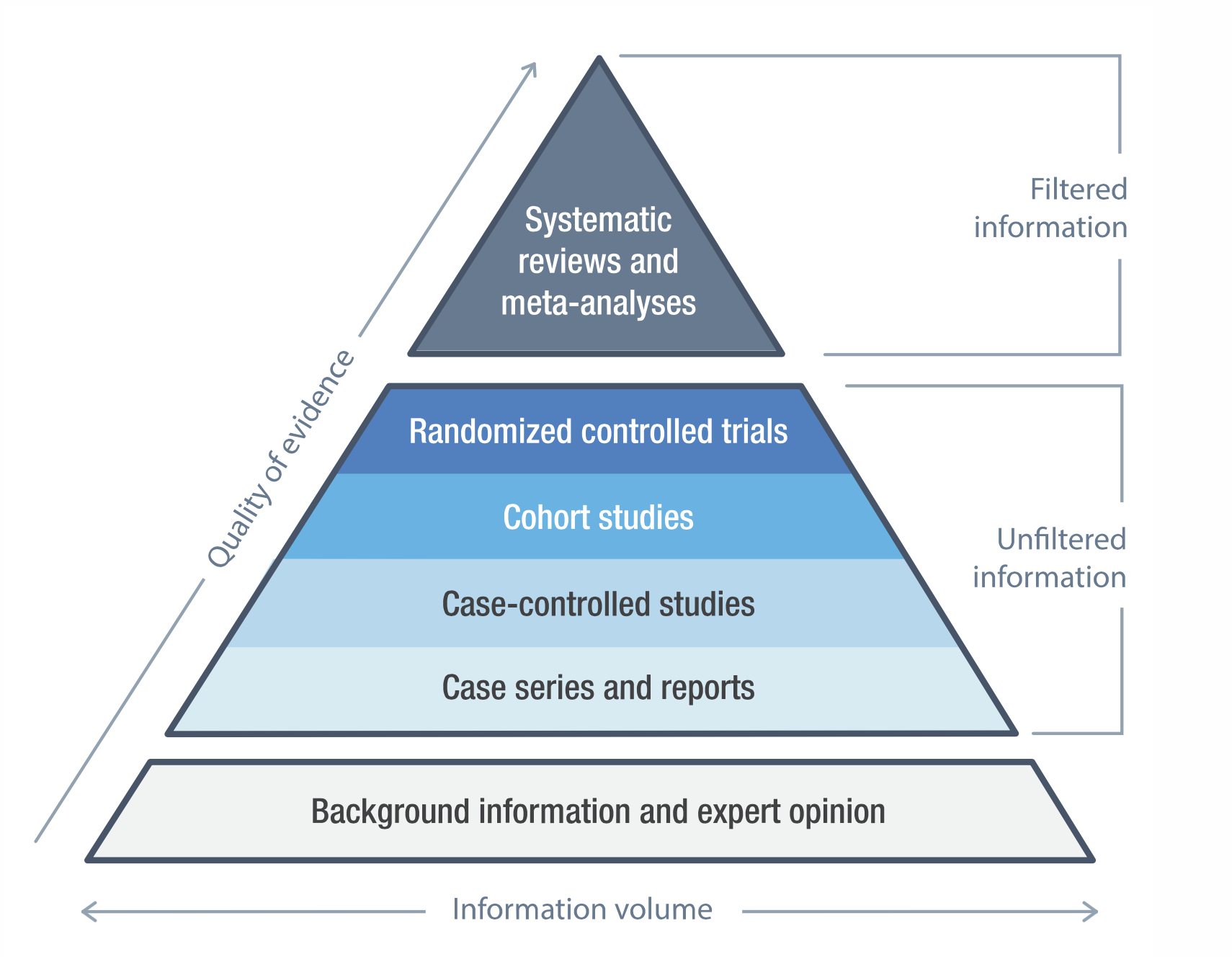
Figure by openmd.com
This approach is rooted in evidence-based medicine (EBM), which is the practice of making medical decisions based on the best available scientific evidence. In this context, “quality of evidence” means that studies:
⬆️ at the top of the pyramid are more reliable because they use strong methods, large groups, and careful controls, while
⬇️ studies at the bottom rely on smaller or less controlled groups.
By following this hierarchy, EBM helps ensure that treatments and recommendations are grounded in solid research rather than anecdote or speculation.
Meta-Analysis
Sormani et al. (2017, Neurology) pooled 15 studies (764 patients, 1995–2016) to estimate mortality, disability progression, and NEDA status after AHSCT. Transplant-related mortality (TRM) averaged 2.1% overall but dropped to 0.3% after 2005. NEDA was reached by 83% of patients at 2 years and 67% at 5 years. Conclusion: AHSCT offers the best risk/benefit ratio in aggressive relapsing-remitting MS (RRMS) with low baseline disability.
🔹Background: MS is often aggressive and refractory to standard DMTs. AHSCT is investigated as an immune reset for severe MS.
🔹Aim: To summarize the evidence on AHSCT for severe and treatment-refractory MS by pooling data (1995–2016) to estimate Transplant-Related Mortality (TRM), disability progression, and No Evidence of Disease Activity (NEDA).
🔹Key Findings:
- Pooled Data: 15 studies with 764 patients.
- TRM: Pooled TRM was 2.1%. TRM was significantly lower in recent studies (0.3% post-2005) and in patients with RRMS and lower baseline disability.
- Efficacy: Progression was 17.1% at 2 years and 23.3% at 5 years. NEDA status was achieved by 83% at 2 years and 67% at 5 years.
🔹Conclusions: AHSCT offers the best benefit/risk profile for patients with aggressive, Relapsing-Remitting MS and low disability. High NEDA rates are superior to most highly effective DMTs, and safety has significantly improved (TRM 0.3% post-2005).
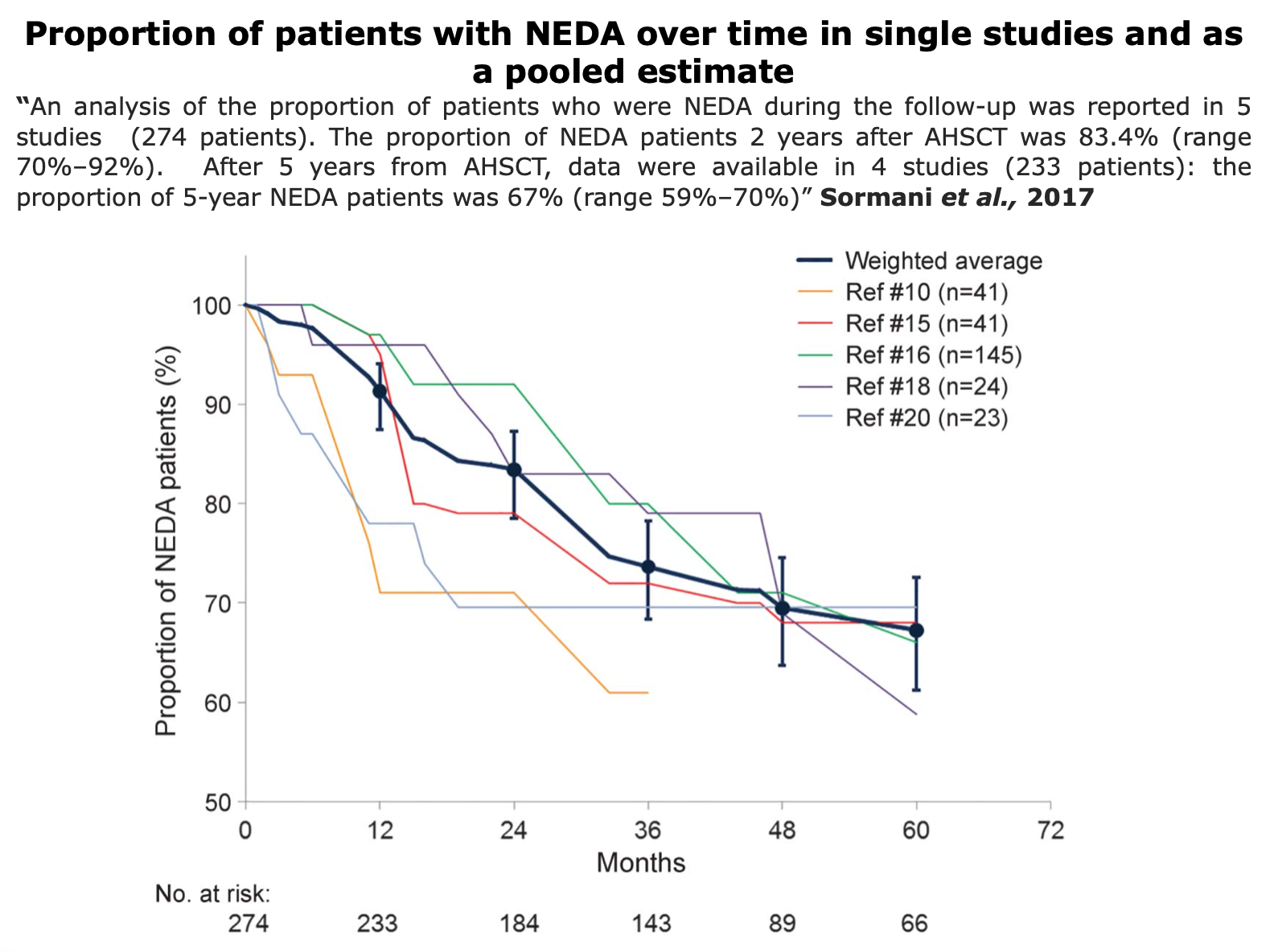
Figure from Sormani et al. “Autologous hematopoietic stem cell transplantation in multiple sclerosis. A meta-analysis”. Neurology (2017)
Systemic Review
RCTs
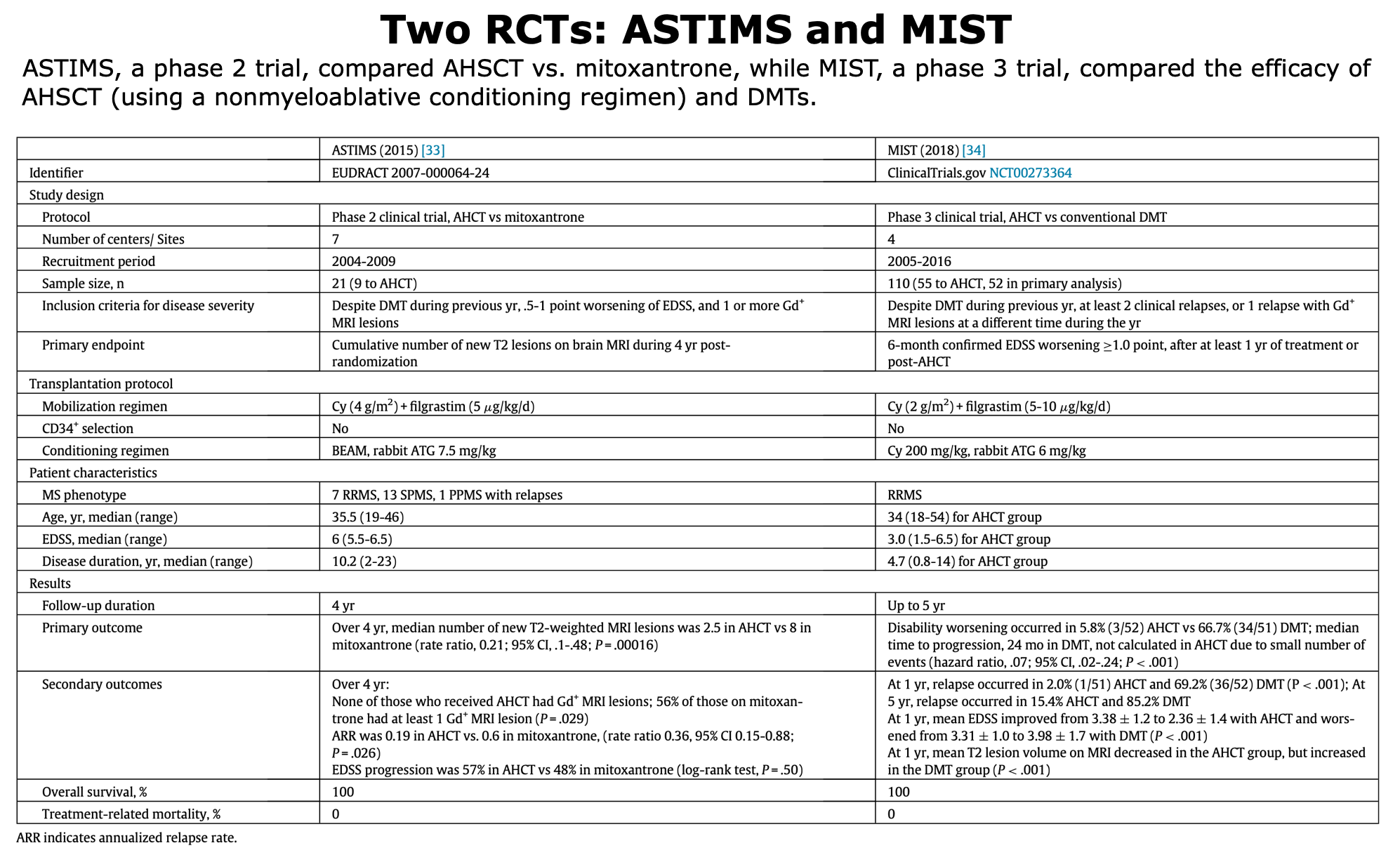
The two completed randomized trials, ASTIMS (2015) and MIST (2018), both showed AHSCT superior to standard therapy (mitoxantrone or various DMTs) in reducing MRI lesions and relapses; MIST also showed disability improvement and better quality of life. Three trials are ongoing (BEAT-MS, RAM-MS, STAR-MS), while three — COAST, MOST and NET-MS— were terminated early due to recruitment and administrative issues rather than safety/efficacy concerns.
1. RCTs completed
ASTIMS (2015) and MIST (2018) are completed RCTs demonstrating superiority of AHSCT over mitoxantrone or various DMTs, though they precede newer agents such as anti-CD20 therapies (ex.: interpreting MIST relapse-free survival outcomes).
Below, the table that summarizes ASTIMS and MIST trial.
Mancardi et al., 2015 “Autologous hematopoietic stem cell transplantation in multiple sclerosis. A phase II trial”. Neurology.
🔹Background: For patients with severe MS who do not respond to standard treatments, intense immunosuppression followed by AHSCT has been proposed to reset the immune system.
🔹Aim: To compare the effect of AHSCT versus mitoxantrone (MTX) on MRI-measured disease activity in patients with severe MS.
🔹Key Findings: AHSCT reduced the number of new T2 MRI lesions by 79% compared to MTX. No patients in the AHSCT group developed new active (Gd+) lesions, compared to 56% in the MTX group. The relapse rate was also significantly lower with AHSCT. However, no significant difference was found in disability progression between the two groups.
🔹Conclusions: AHSCT is significantly superior to MTX in suppressing inflammatory MRI activity in severe MS. The results strongly support further studies to evaluate AHSCT’s effect on clinical endpoints.
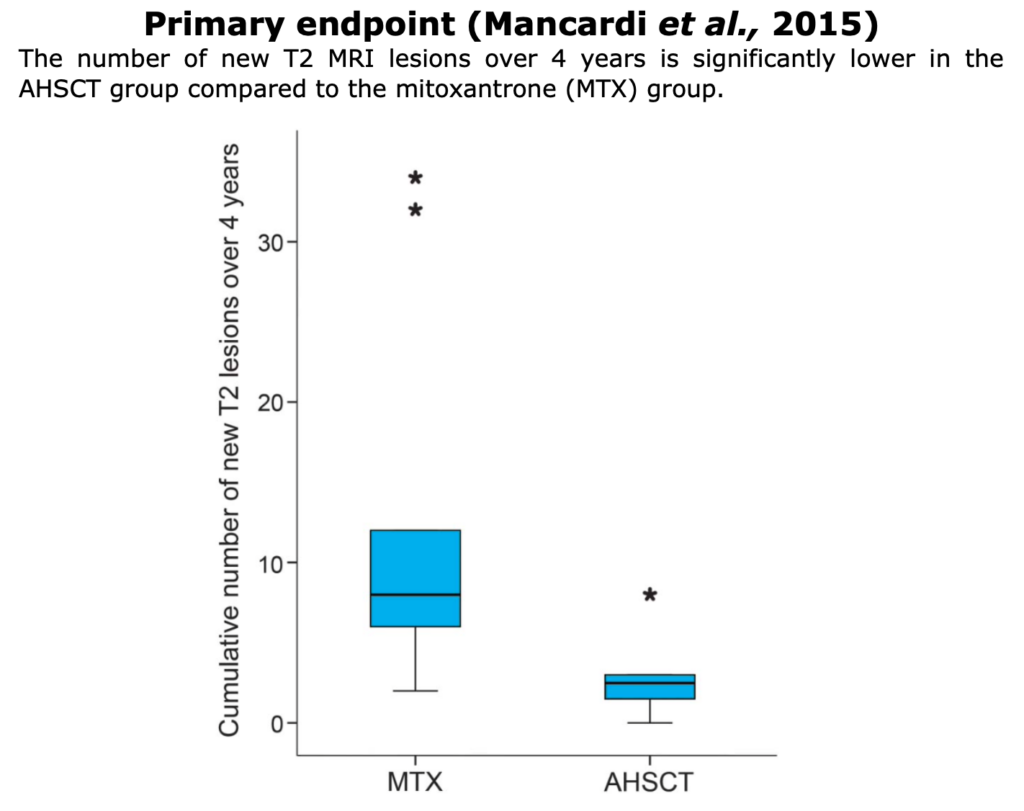
Figure from Mancardi et al. “Autologous hematopoietic stem cell transplantation in multiple sclerosis A phase II trial”. Neurology (2015).
Burt et al., 2019 “Effect of Nonmyeloablative Hematopoietic Stem Cell Transplantation vs Continued Disease-Modifying Therapy on Disease Progression in Patients With Relapsing-Remitting Multiple Sclerosis. A Randomized Clinical Trial”. JAMA
🔹Background: Standard DMTs are often insufficient for controlling highly active RRMS. AHSCT is a therapy designed to reset the immune system.
🔹Aim: To compare the effectiveness of nonmyeloablative AHSCT versus DMT on disease progression in patients with active RRMS.
🔹Key Findings: Disease progression occurred in 3 HSCT patients versus 34 DMT patients (Hazard Ratio, 0.07). In the first year, disability scores (EDSS) improved in the HSCT group but worsened in the DMT group. The relapse rate was 2% in the HSCT group versus 69% in the DMT group. No deaths or major toxicities occurred in the HSCT group.
🔹Conclusions: In patients with active RRMS, AHSCT was significantly more effective than DMT at preventing disease progression and improving disability.
2. RCTs - Ongoing Trials
To date, there are 4 ongoing trials. For more information, please visit the following links: BEAT-MS, RAM-MS trial and STAR-MS.
For the section dedicated to trials on this website, click here and here for an overview.
3. RCTs - Terminated
Some trials do not reach publication due to operational, methodological, or recruitment constraints. NET-MS ended due to feasibility (recruitment issues), MOST ended following the principal investigator’s sabbatical, and COAST stopped due to low acceptance of the control arm.
Observational Prospectives
🔹Background: AHSCT is an emerging treatment for highly active RRMS. However, there is limited evidence on the long-term role of DMTs after AHSCT.
🔹Aim: To evaluate long-term outcomes of MS patients treated with AHSCT in Lithuania from May 2014 to January 2025 and to explore treatment strategies, including the use of DMT, in those with disease activity after transplantation.
🔹Key findings: Forty-two RRMS patients underwent AHSCT with a median follow-up of 65 months. 65% achieved sustained NEDA-3, and 35% showed early and lasting improvement in disability. About 29% required additional DMT post-AHSCT, mostly ocrelizumab or siponimod, which proved effective in stabilizing disease in several cases. No treatment-related mortality occurred.
🔹Conclusions: AHSCT provided durable disease control and disability improvement in the majority of patients with highly active RRMS. For those with residual disease activity, high-efficacy DMTs remained a safe and effective option. These findings reinforce AHSCT as a strong therapeutic strategy, with DMTs serving as a valuable complement in selected cases.
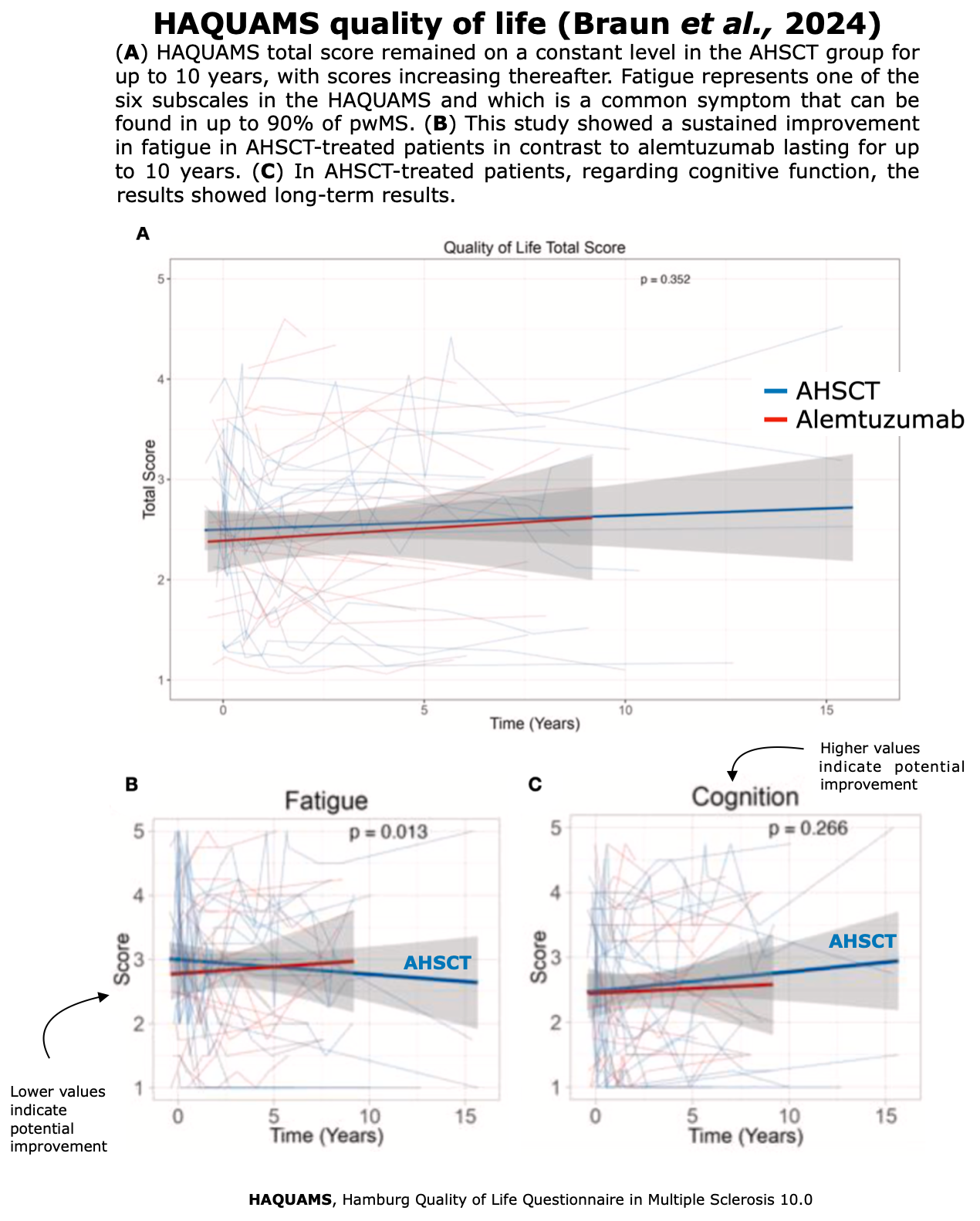
Braun et al., 2024. “Benefits of AHSCT over alemtuzumab in patients with multiple sclerosis besides disability and relapses: Sustained improvement in cognition and quality of life”. Multiple Sclerosis and Related Disorders
This monocentric study provides an update of the data published in 2021 by Häußler et al.
🔹Background: MS often progresses despite DMTs. AHSCT is highly effective short-term, but long-term data on cognition and QoL are scarce. Alemtuzumab is another induction therapy with limited durability.
🔹Aim: Compare long-term outcomes of AHSCT vs. alemtuzumab in highly active MS.
🔹Key Findings:
- NEDA-3: Higher rates with AHSCT (75% at 5 years; 55% at 10 years) vs. alemtuzumab (40% at 5 years).
- Relapses and MRI activity: Relapse-free survival and absence of new T2 lesions were significantly more frequent in the aHSCT group.
- Cognition: AHSCT patients improved in 5/12 cognitive domains (attention, processing speed, verbal learning, divided attention), whereas alemtuzumab patients declined in 4/12 domains.
- Quality of life: AHSCT maintained stable QoL for up to 10 years, with improved fatigue scores, while alemtuzumab patients reported deterioration.
- EDSS: Similar progression overall, but more AHSCT patients showed confirmed improvements.
- Safety: Both treatments carried risks, but adverse events were manageable; no treatment-related mortality was observed in the AHSCT cohort.
🔹Conclusions: AHSCT is superior to alemtuzumab in maintaining long-term disease inactivity, improving cognition, and preserving QoL for up to a decade. These findings support considering AHSCT as a strong therapeutic option for highly active MS, though larger controlled trials are needed.
 Figures from Braun et al. “Benefits of AHSCT over alemtuzumab in patients with multiple sclerosis besides disability and relapses: Sustained improvement in cognition and quality of life”. Multiple Sclerosis and Related Disorders (2024)
Figures from Braun et al. “Benefits of AHSCT over alemtuzumab in patients with multiple sclerosis besides disability and relapses: Sustained improvement in cognition and quality of life”. Multiple Sclerosis and Related Disorders (2024)
Burt et al., 2022 “Real‐world application of autologous hematopoietic stem cell transplantation in 507 patients with multiple sclerosis”. Journal of Neurology.
🔹Background: AHSCT has shown efficacy in RRMS, but its role in SPMS and long-term real-world safety remain less clear.
🔹Aim: To report real-world outcomes of non-myeloablative AHSCT in 507 MS patients (414 RRMS, 93 newly diagnosed SPMS) treated at Northwestern University between 2003–2019.
🔹Key Findings:
- Survival/safety: 5-year overall survival 98.8%; treatment-related mortality 0.19% (1 death from legionella pneumonia).
- Secondary autoimmunity: 10 ITP cases (2–3% non-alemtuzumab vs. 11.5% with alemtuzumab), ~7% thyroid disorders.
- Relapse-free survival (RFS): RRMS 80.1% at 5y; SPMS 98.1% at 5y.
- Progression-free survival (PFS): RRMS 95% at 4y vs. SPMS 66% at 4y.
- Disability (EDSS): RRMS improved from 3.87 to 2.19 at 5y (p<0.0001). SPMS improved slightly at 1y (5.09→4.85, p=0.04) but not sustained.
🔹Conclusions: Non-myeloablative AHSCT is a safe and highly effective one-time therapy for RRMS, producing durable relapse and progression control with significant EDSS improvement. Benefit in SPMS is limited, especially without active inflammation.

Figure from Burt et al. “Real‐world application of autologous hematopoietic stem cell transplantation in 507 patients with multiple sclerosis”. Journal of Neurology (2022)
The study by Braun et al., 2024 was based on an update of the data published in 2021 by Häußler et al. (“AHSCT is superior to alemtuzumab in maintaining NEDA and improving cognition in multiple sclerosis”) published in Annals of Clinical and Translational Neurology.
🔹Background: AHSCT can reset the immune system in MS and may be more effective than high-efficacy DMTs like alemtuzumab, but direct comparisons are scarce.
🔹Aim: To compare outcomes of AHSCT vs. alemtuzumab in MS patients regarding NEDA, disability, and cognition.
🔹Key Findings:
- Cohort: 19 AHSCT vs. 21 alemtuzumab patients, mean follow-up 59 vs. 28 months.
- NEDA: 62% with AHSCT vs. 40% with alemtuzumab (p=0.038).
- EDSS: 37% of AHSCT improved vs. 0% with alemtuzumab (p=0.033).
- Relapses/MRI: No relapses or MRI activity in aHSCT group; 51% alemtuzumab patients developed new T2 lesions.
- Cognition: AHSCT improved attention/processing speed, while alemtuzumab patients declined across domains.
- Safety: Mostly expected early infections; one death (CML, linked to prior mitoxantrone), isolated thyroid disease, polyarthritis, infertility.
🔹Conclusions: AHSCT more effectively suppresses inflammatory activity and supports disability and cognitive improvement compared to alemtuzumab. It appears safe and promising for highly active MS, especially in RRMS.
Hamerschlak et al.. “Brazilian experience with two conditioning regimens in patients with multiple sclerosis: BEAM/horse ATG and CY/rabbit ATG”. BMT
🔹Background: AHSCT is an intensive immunosuppressive therapy used to prevent disease progression in patients with refractory MS. Controversy exists regarding the ideal conditioning regimen, particularly concerning the safety and efficacy of more intensive (myeloablative) versus less intensive (non-myeloablative) approaches.
🔹Aim: This prospective Brazilian study aimed to compare the toxicity and clinical outcomes of two different conditioning regimens used for HSCT in MS patients: an intermediate-intensity regimen (BEAM with horse ATG) and a non-myeloablative regimen (Cyclophosphamide with rabbit ATG)
🔹Key Findings:
- The study included 41 patients, most of whom had secondary progressive MS (80.4%) and significant disability, with 78% having a baseline EDSS score of 6.0 or higher.
- The protocol was changed from BEAM/horse ATG to CY/rabbit ATG after the first 21 patients because of an unacceptable mortality rate; three patients (7.5% of the total) died in the BEAM/ATG group, whereas there were no deaths in the CY/ATG group.
- The BEAM/ATG regimen was significantly more toxic, resulting in more complications during transplantation (71.4% vs. 40%), longer hospital stays, and a greater need for blood and platelet transfusions compared to the CY/ATG regimen.
- Despite the differences in toxicity, the efficacy was similar between the two groups. Overall, 63.2% of patients remained stable or improved. Event-free survival (EFS) showed no statistically significant difference between the BEAM group (47%) and the CY group (70%).
- After transplantation, no new enhancing lesions were seen on MRI in any patient from either group.
🔹Conclusions: In this study, the non-myeloablative CY/rabbit ATG regimen was associated with significantly less toxicity and appeared to be as effective as the more intensive BEAM/horse ATG regimen. Although long-term follow-up is required for a full assessment, the CY/rATG regimen demonstrated a better safety profile for this patient population.
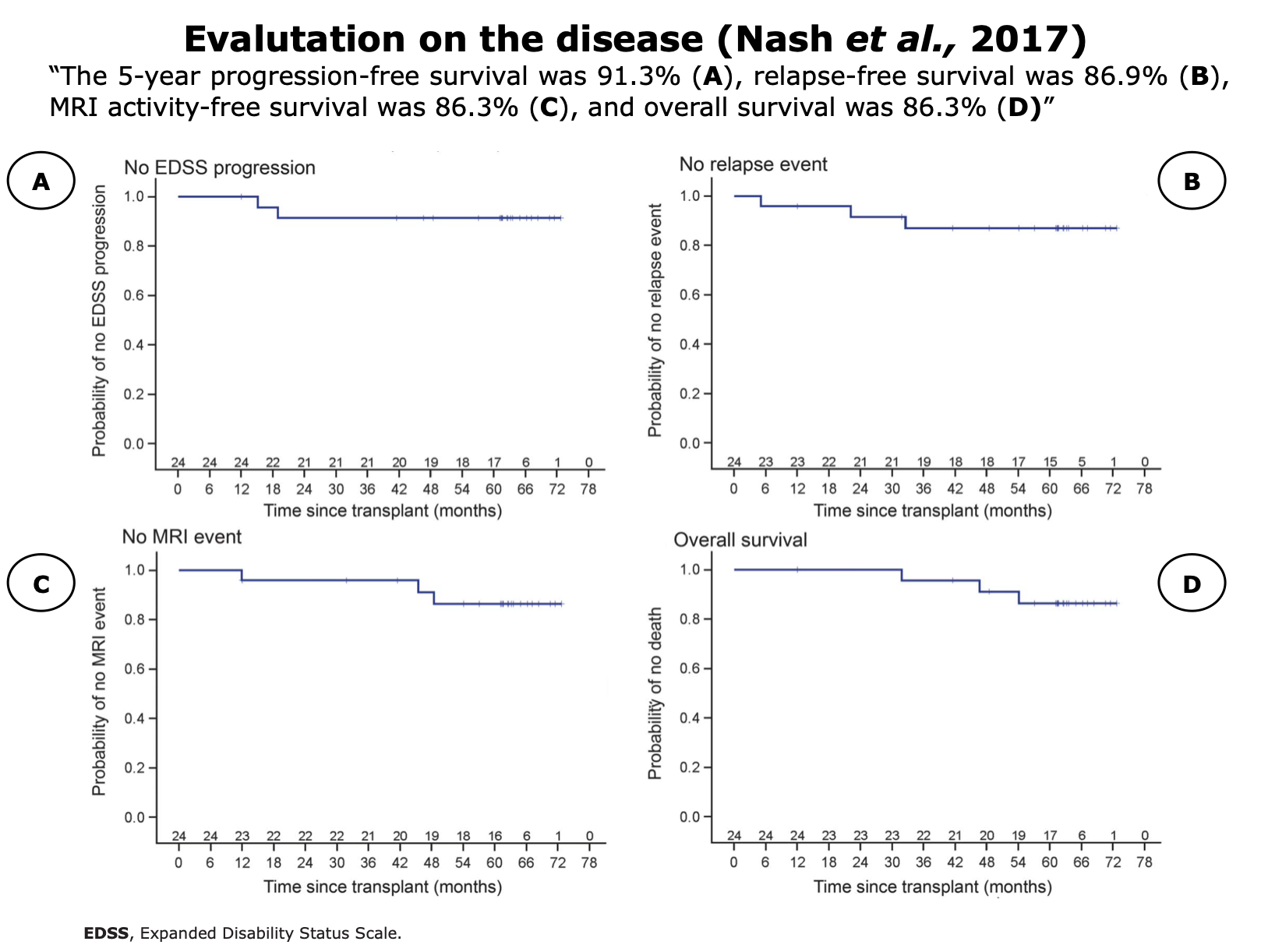
Nash et al. “High-dose immunosuppressive therapy and autologous HCT for relapsing-remitting MS”. Neurology
🔹Background: The HALT-MS trial investigated if high-dose immunosuppressive therapy (HDIT) followed by AHSCT could reset the immune system to control active RRMS in patients who did not respond to standard therapies.
🔹Aim: The study’s goal was to assess the 5-year safety and effectiveness of HDIT/HCT in inducing durable disease stabilization for patients with RRMS. The primary endpoint was event-free survival (EFS), defined as survival without death, disability progression, relapse, or new MRI lesions.
🔹Key Findings:
- 24 patients underwent the procedure and were followed for a median of 62 months.
- At 5 years, the event-free survival rate was 69.2%.
- Progression-free survival was 91.3%, and relapse-free survival was 86.9%.
- Surviving patients who completed the study showed neurological improvement, with a median EDSS score reduction of 0.5.
- Adverse events were as expected for this type of procedure, and no deaths were attributed to the transplant.
🔹Conclusions: HDIT/HCT, as a one-time treatment without ongoing therapy, was effective in inducing long-term, sustained remission of active RRMS at 5 years. It represents a potential therapeutic option for patients with RRMS who fail conventional treatments.
Figures from Nash et al. “High-dose immunosuppressive therapy and autologous HCT for relapsing-remitting MS”. Neurology (2017)
Propensity Score
🔹Background: Progression independent of relapse activity (PIRA)—the gradual worsening of disability not linked to relapses—is a major cause of long-term disability in MS and is poorly controlled by standard disease-modifying treatments (DMTs). Since the chemotherapy used in AHSCT reaches the central nervous system, it may also act on the mechanisms driving PIRA.
🔹Aim: To To compare the long-term effects of AHSCT versus natalizumab (NTZ) and subsequent DMTs on PIRA in aggressive RRMS.
🔹Key Findings:
In a matched study of 30 AHSCT and 30 NTZ-treated patients (median follow-up 106 months), PIRA rates were similar during NTZ therapy but significantly lower after AHSCT over the full follow-up (10% vs 49% at 10 years, p=0.020). AHSCT also outperformed controls in reducing relapses, overall disability progression, and achieving no evidence of disease activity (NEDA-3). Conversion to secondary-progressive MS occurred in 7% after AHSCT versus 40% after NTZ.
🔹Conclusions: AHSCT substantially reduced long-term disability progression unrelated to relapses (PIRA) in aggressive RRMS compared with DMTs. Early intervention targeting both peripheral and central nervous system inflammation may best prevent irreversible disease progression.
🔹Limitations: In this study, anti-CD20 were not compared with AHSCT.
Kalincik et al., 2025. “Effectiveness of autologous haematopoietic stem cell transplant in comparison with anti-CD20 therapies in relapsing-remitting MS“. Poster ECTRIMS 2025.
🔹Background: AHSCT may offer stronger disease control for MS patients who respond suboptimally to high-efficacy immunotherapies (e.g. anti-CD20). Head-to-head evidence comparing these approaches is lacking.
🔹Aim: To emulate a comparative effectiveness trial of AHSCT versus anti-CD20 therapies (ocrelizumab, rituximab) in RRMS.
🔹Key Findings:
- Cohort: The study included matched cohorts of 152 AHSCT-treated patients and 859 anti-CD20-treated patients (ocrelizumab 752 and rituximab 107 patients).
. Both groups had highly active MS (79–82% with relapses in the prior 2 years) and moderate disability (mean EDSS > 3.5). - Relapse Suppression: AHSCT was associated with a significantly lower risk of relapses (Annualized Relapse Rate 0.04 vs. 0.09; p<0.0001) compared to anti-CD20 therapy.
- Disability: AHSCT showed a similar risk of confirmed disability worsening but a higher probability of confirmed disability improvement (Hazard Ratio 1.91) than anti-CD20 therapy.
- Safety: AHSCT was associated with a risk of infections, but no treatment-associated deaths (TRM) were reported in the AHSCT group.
🔹Conclusions: In patients with active RRMS and moderate disability, AHSCT outperforms anti-CD20 therapy (ocrelizumab, rituximab) in suppressing relapses and promoting recovery of neurological function, with comparable risk of disability worsening and acceptable safety in this cohort.
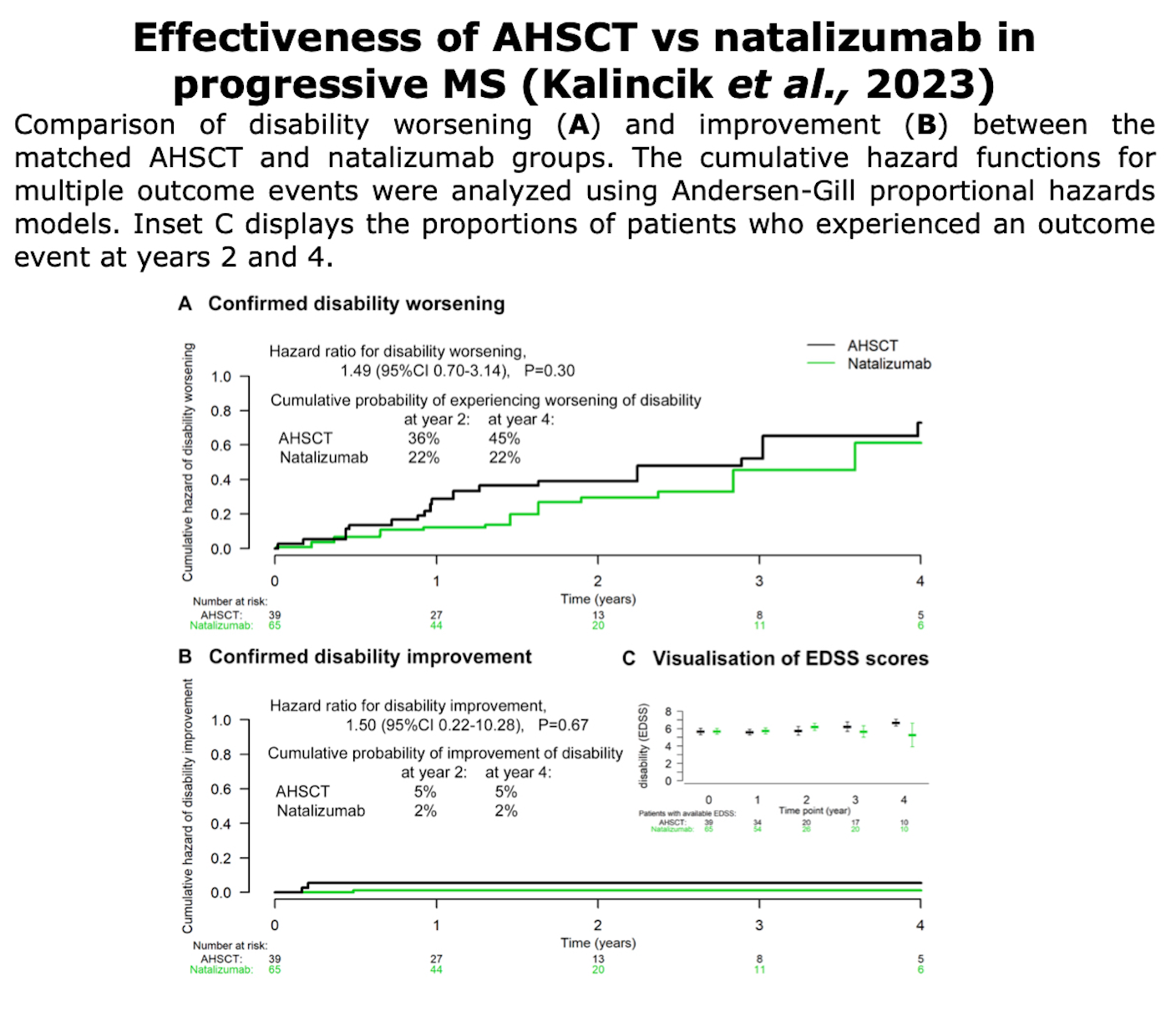
Kalincik et al., 2024. “Effectiveness of autologous haematopoietic stem cell transplantation versus natalizumab in progressive multiple sclerosis”. Journal of Neurology, Neurosurgery & Psychiatry.
🔹Background: Natalizumab has not demonstrated clear benefit in modifying disability progression in progressive forms of multiple sclerosis. AHSCT is proposed as an alternative, but comparative data are limited.
🔹Aim: To compare AHSCT with natalizumab in patients with primary or secondary progressive MS, specifically looking at relapse rates, disability worsening and improvement over follow-up of up to ~4 years.
🔹Key Findings:
- Sample: 39 patients treated with AHSCT (mostly secondary progressive MS; mean age ~37; mean EDSS ~5.7; about 28% had recent disability progression) matched with 65 treated with natalizumab.
- Pre-treatment relapse rate for the AHSCT group was high (~0.54/year), but during treatment both groups had low relapse rates (~0.08/year).
- No significant difference between AHSCT and natalizumab in risk of confirmed disability worsening (HR ~1.49) or confirmed disability improvement (HR ~1.50).
- Relapse activity while on treatment was similar for both (ARR ~0.08).
- Safety: In the AHSCT group there were multiple complications (febrile neutropenia, serum sickness, ICU admissions, post-discharge complications), but no treatment-related deaths.
🔹Conclusions: In progressive MS patients with advanced disability and low relapse activity, AHSCT was not clearly superior to natalizumab in preventing disability worsening, promoting improvement, or reducing relapse frequency. Given risks, AHSCT is not supported over natalizumab in this subgroup.
Figures from Kalincik et al. ”Effectiveness of autologous haematopoietic stem cell transplantation versus natalizumab in progressive multiple sclerosis“. J Neurol Neurosurg Psychiatry (2024)
Boffa et al., 2023. “Hematopoietic Stem Cell Transplantation in People With Active Secondary Progressive Multiple Sclerosis”. Neurology
🔹Background: SPMS with residual inflammatory activity remains challenging to treat. While AHSCT has shown strong efficacy in relapsing-remitting MS, evidence in active SPMS is limited.
🔹Aim: To compare AHSCT with conventional DMTs in active SPMS using real-world data from the Italian BMT-MS Study Group and MS Register.
🔹Key Findings:
- Cohorts: 79 AHSCT (14 centers) vs 1,975 DMT-treated patients (IFN-β, GA, AZA, MTX, CYC, MITX, FTY, NAT, ALM, DMF, TER); matched subset: 69 vs 345.
- Relapses: ARR 0.02 vs 0.43 → ~95% reduction (p<0.001).
- Disability progression: HR 0.50 (95% CI 0.31–0.81; p=0.005) → half the risk of EDSS worsening (50% lower risk of sustained EDSS worsening).
- Disability improvement: HR 4.21 (p<0.001) → ~4× higher chance of EDSS recovery.
- Safety: One treatment-related death (1.3%).
- NEDA-3/QoL: not evaluated.
🔹Conclusions: In active SPMS, AHSCT demonstrated statistically superior efficacy over conventional DMTs across all evaluated outcomes—marked relapse suppression, reduced disability progression, and increased probability of improvement.
However, the study is observational (Class III), lacks modern comparators (e.g., ocrelizumab, siponimod), and carries higher procedural risk.
AHSCT appears the most potent option for selected active-SPMS patients, but requires careful risk-benefit assessment and prospective validation.
Kalincik et al., 2023 “Comparative Effectiveness of Autologous Hematopoietic Stem Cell Transplant vs Fingolimod, Natalizumab, and Ocrelizumab in Highly Active Relapsing-Remitting Multiple Sclerosis”. American Medical Association
🔹Background: AHSCT is an intensive immune-reconstitution therapy for highly active RRMS when standard treatments are not enough.
🔹Aim: To compare effectiveness of AHSCT vs three disease-modifying therapies (fingolimod, natalizumab, ocrelizumab) in reducing relapses and/or improving disability in highly active RRMS.
🔹Key Findings:
- AHSCT showed much lower relapse rates than fingolimod; slightly lower than natalizumab.
- Disability improvement was greater with AHSCT vs fingolimod and natalizumab.
- No clear difference between AHSCT and ocrelizumab over the shorter follow-up period.
- Treatment-related mortality from AHSCT was low (~0.6%), though there were serious adverse events.
🔹Conclusions: AHSCT is more effective than fingolimod, and somewhat better than natalizumab, for relapse prevention and disability recovery in highly active RRMS. Its benefits vs ocrelizumab are uncertain given current follow-up. Though higher risk, its one-off nature may favour its use in selected patients.
Table from Kalincik et al. “Comparative Effectiveness of Autologous Hematopoietic Stem Cell Transplant vs Fingolimod, Natalizumab, and Ocrelizumab in Highly Active Relapsing-Remitting Multiple Sclerosis”. JAMA Neurology (2023)
Mariottini et al., 2022. “Autologous haematopoietic stem cell transplantation versus low-dose immunosuppression in secondary–progressive multiple sclerosis”. European Journal of Neurology
🔹Background:
- AHSCT has proven efficacy in relapsing–remitting MS, but its role in SPMS is less clear.
- Low-dose immunosuppression with intravenous Cy is used as a treatment in SP-MS, particularly where high-efficacy options are limited.
🔹Aim: To compare the long-term effectiveness and safety of intermediate-intensity AHSCT vs low-dose immunosuppression with IV cyclophosphamide in patients with SP-MS, matched on baseline characteristics.
🔹Key Findings:
- Sample: 93 SP-MS patients (31 AHSCT, 62 Cy), mean follow-up ~99 months for AHSCT, ~91 months for Cy.
- Relapse-free survival (R-FS): At 5 years, 100% in AHSCT vs ~52% in Cy group. AHSCT fully suppressed relapses.
- Disability progression (P-FS): No statistically significant difference at 5 years (≈70% AHSCT vs ≈81% Cy).
- Other disability outcome (worsening confirmed) also similar between groups.
- NEDA-2 (no evidence of disease activity type 2: no relapses + no confirmed EDSS worsening): no significant difference.
- Safety: 1 cancer in AHSCT vs 2 in Cy; 2 deaths occurred in Cy group; none in AHSCT.
🔹Conclusions:
- In SPMS, AHSCT is markedly superior to cyclophosphamide for suppressing relapses.
- However, AHSCT did not show clear benefit over Cy in preventing disability accrual in this cohort.
- This suggests that, in SPMS, disability progression may be driven more by neurodegeneration (less responsive to immunotherapy) than by active inflammation.
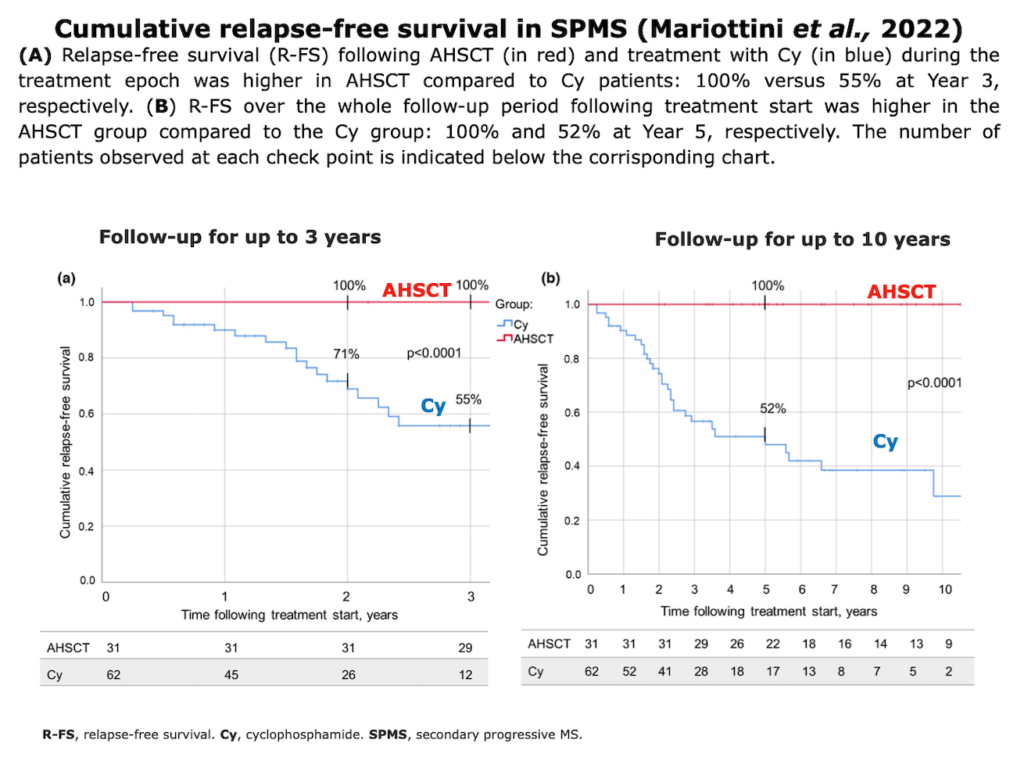
Mariottini et al. “Autologous haematopoietic stem cell transplantation versus low-dose immunosuppression in secondary–progressive multiple sclerosis”. European Journal of Neurology (2022)
Observational Retrospectives
Kalincik et al., 2026: “Haematopoietic stem cell transplant versus immune-reconstitution therapy in relapsing multiple sclerosis“. Brain
🔹Background: AHSCT and immune-reconstitution therapies (IRTs) share mechanistic similarities and are used in highly active relapsing MS, but direct, head-to-head comparative clinical data were completely lacking.
🔹Aim: To compare the real-world clinical effectiveness of AHSCT versus the IRTs cladribine and alemtuzumab in relapsing-remitting multiple sclerosis (RRMS) patients using emulated pairwise trials from international registries.
🔹Key findings: AHSCT significantly reduced the annualized relapse rate compared to both cladribine (HR 0.24) and alemtuzumab (HR 0.52). While no significant differences were observed regarding confirmed disability worsening, AHSCT was markedly superior in facilitating 6-month confirmed disability improvement (HR 2.19 vs cladribine; HR 2.03 vs alemtuzumab). Delayed complications (mostly infections) affected 34% of the AHSCT cohort, but zero treatment-related deaths occurred. Sensitivity analyses confirmed the robustness of the cladribine comparison, whereas the alemtuzumab cohort was more susceptible to residual, unmeasured confounding.
🔹Conclusions: In active RRMS with moderate disability, AHSCT surpasses both cladribine and alemtuzumab in suppressing clinical relapses and promoting short-term neurological recovery, without exposing patients to a higher risk of disability progression. The superior therapeutic value of AHSCT over established IRTs likely stems from the unique depth of immune ablation and qualitative immune reconstitution achieved during the transplantation procedure.
Muraro et al., 2025. “Effectiveness of Autologous Hematopoietic Stem Cell Transplantation versus Alemtuzumab and Ocrelizumab in Relapsing Multiple Sclerosis: A Single Center Cohort Study“. Annals of Neurology
🔹Background: Real-world comparative evidence for AHSCT against high-efficacy disease-modifying therapies (DMTs), particularly anti-CD20 agents, remains scarce due to small cohort sizes, heterogeneous protocols, and the lack of robust MRI data.
Muraro et al. “Real-world effectiveness of autologous haematopoietic stem cell transplantation for multiple sclerosis in the UK“. J Neurol Neurosurg Psychiatry.
🔹Background: AHSCT is increasingly used as a potentially definitive, one-off disease-modifying therapy for aggressive forms of MS. This study reports the real-world effectiveness of AHSCT based on the nationwide experience in the UK.
🔹Aim: The objective was to report the real-world effectiveness of AHSCT by assessing long-term outcomes, including relapse-free survival (RFS), MRI activity-free survival (MFS), progression-free survival (PFS), and NEDA-3, in a large, unselected cohort of UK patients.
🔹Key Findings:
- Cohort: The study included 364 patients treated between 2002 and 2023. Among those with adequate follow-up data (n=271), 62% had RRMS and 38% had Progressive MS (PMS). The median baseline EDSS score was 6.0, indicating significant disability.
- Long-term Efficacy (at 5 years):
- Relapse-Free Survival (RFS) was 88.6%.
- MRI Activity-Free Survival (MFS) was 80.1%.
- Progression-Free Survival (PFS) was 62.4%.
- NEDA-3 was 46.2%.
- Disability Status: RRMS patients had significantly higher rates of NEDA-3 and PFS than PMS patients. The prevalence of EDSS improvement was 20.4% at 5 years, with RRMS being a predictor of this improvement.
- Safety: Treatment-related mortality (TRM), defined as death within 100 days, was 1.4% (n=5/364).
🔹Conclusions: In this large, real-world UK cohort, AHSCT led to durable remission of inflammatory activity and resulted in stabilization or improvement of neurological disability. The procedure proved particularly effective in patients with RRMS, supporting AHSCT as a highly effective option for aggressive MS.
Kazmi et al., 2025. “Autologous haematopoietic stem cell transplantation for multiple sclerosis in the UK: A 20-year retrospective analysis of activity and haematological outcomes from the British Society of Blood and Marrow Transplantation and Cellular Therapy (BSBMTCT)“. B J Haem.
🔹Background: AHSCT has been developed since 1995 as an intensive immune “reset” therapy for MS. The UK is among the most active countries performing AHSCT for MS, but access remains uneven across regions.
🔹Aim: To describe national UK outcomes and safety of AHSCT for MS over 20 years (2002–2023) and identify factors influencing efficacy and complications.
🔹Key Findings:
- Cohort: 364 patients (58% RRMS, 36% progressive MS); median age 40 years; median EDSS 6.0; median disease duration 10 years.
- Efficacy: Progression-free survival (PFS) was 83.5% at 2 years and 62.4% at 5 years. RRMS patients had significantly better PFS than SPMS or PPMS (HR 1.69–2.07).
- Safety: Transplant-related mortality (TRM) 1.4%, all in patients with advanced disability (median EDSS 6.5).
- Complications: EBV reactivation in 76%, CMV in 21%; significant viral reactivation and higher ATG doses (>6 mg/kg) correlated with reduced PFS.
- Long-term events: Secondary autoimmune diseases (7.9%), mostly thyroiditis; malignancies in 1.6%.
- Geography: 88% of transplants occurred after 2016, mainly in London and Sheffield; limited access in other UK regions.
🔹Conclusions: AHSCT is an effective and increasingly safe one-off treatment for severe or refractory MS, yielding durable disease control, particularly in RRMS. Outcomes worsen with higher disability, progressive disease, and excessive ATG dosing. The study supports limiting ATG to ≤6 mg/kg and expanding equitable AHSCT access across the UK.
🔹Background: AHSCT is an increasingly used treatment for aggressive RRMS. Despite strong efficacy signals, controlled data remain limited; therefore, national real-world experiences are valuable for assessing safety and effectiveness.
🔹Aim: To describe the Danish nationwide experience with AHSCT for aggressive RRMS regarding patient characteristics, safety, and efficacy.
🔹Key Findings:
- Cohort: 32 RRMS patients (median age 36 years; median EDSS 3.5–5.0) treated from 2011–2021. Seven received BEAM/ATG, and 25 received cyclophosphamide (CY)/ATG.
- Efficacy: At 2 years, relapse-free survival (RFS) was 77%, worsening-free survival (WFS) 79%, MRI event-free survival (MFS) 93%, and NEDA-3 69%. CY/ATG showed higher efficacy (NEDA-3 77%) than BEAM/ATG (43%).
- Safety: No treatment-related mortality; most adverse events were mild to moderate. BEAM caused more acute and late AEs than CY.
- Complications: Viral reactivations (EBV 24–43%, CMV <10%), thyroid autoimmunity (up to 28%), and herpes zoster (mainly post-prophylaxis). One unrelated death occurred 6 years post-transplant.
- Regimen comparison: CY/ATG was equally or more effective than BEAM, with fewer severe AEs and lower toxicity.
🔹Conclusions: AHSCT is a highly effective and safe treatment for aggressive RRMS, achieving durable NEDA in most patients without mortality. The Danish experience supports CY/ATG as the preferred regimen due to similar efficacy and superior safety, while confirming the need for randomized trials versus high-efficacy DMTs.
Boffa et al., 2021 “Long-term Clinical Outcomes of Hematopoietic Stem Cell Transplantation in Multiple Sclerosis”. Neurology
🔹Background: Current DMTs for MS are often insufficient to prevent long-term disability progression. AHSCT has been investigated as an aggressive strategy to eliminate autoreactive immune cells and induce drug-free self-tolerance in patients with highly active MS. Long-term, real-world data confirming durable remission were needed.
🔹Aim: The objective was to determine, through the analysis of a large, multicenter cohort of aggressive MS patients, whether AHSCT is capable of inducing durable disease remission and preventing long-term disability worsening.
🔹Key Findings: The study included 210 MS patients (58% with RRMS) with a mean follow-up of 6.2 years.
- Disability Worsening-Free Survival (DWFS): For RRMS patients, DWFS was 85.5% at 5 years and 71.3% at 10 years. Progressive MS patients had a lower DWFS (71.0% at 5 years; 57.2% at 10 years).
- Disability Status: RRMS patients showed a significant reduction in EDSS score over time (p=0.001).
- NEDA-3 Status: The probability of maintaining NEDA-3 in RRMS was 62.2% at 5 years and 40.5% at 10 years.
- Conditioning Protocol: The BEAM + Anti-thymocyte globulin (ATG) protocol was independently associated with a significantly reduced risk of NEDA-3 failure in RRMS (HR 0.27, p<0.001).
- Safety: Transplantation-related mortality was 1.4% (3 patients) and zero for patients transplanted after 2007.
🔹Conclusions: AHSCT is effective in preventing long-term disability worsening and inducing durable clinical improvement, particularly in patients with RRMS. The BEAM + ATG conditioning protocol offers superior suppression of clinical and radiological inflammatory activity. The study supports AHSCT as a viable option for inducing long-term, drug-free remission in appropriately selected MS patients.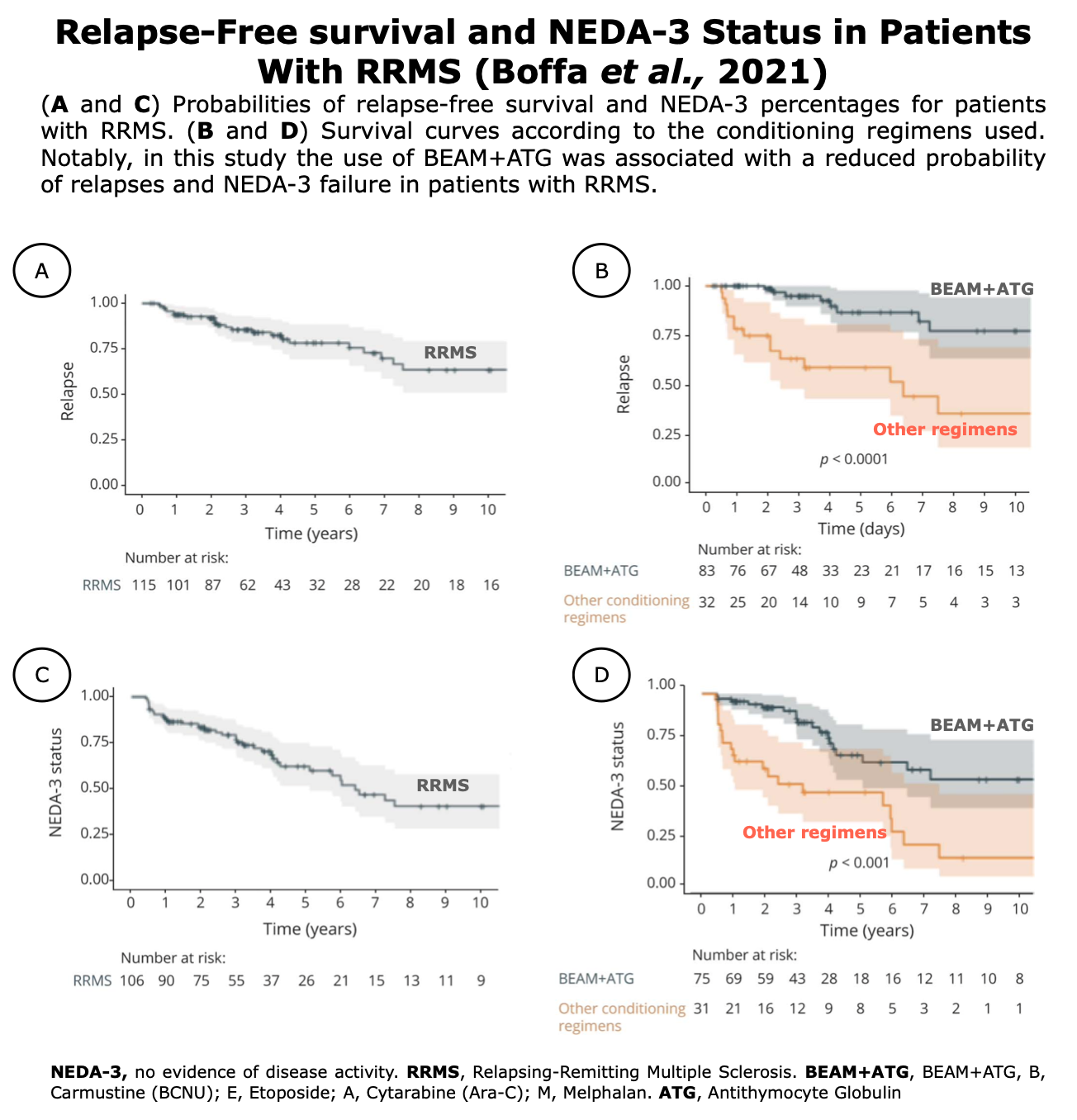 Figures from Boffa et al. “Long-term Clinical Outcomes of Hematopoietic Stem Cell Transplantation in Multiple Sclerosis”. Neurology (2021)
Figures from Boffa et al. “Long-term Clinical Outcomes of Hematopoietic Stem Cell Transplantation in Multiple Sclerosis”. Neurology (2021)
Das et al., 2021. “Autologous haematopoietic stem cell transplantation as a first-line disease-modifying therapy in patients with “aggressive” multiple sclerosis”. Multiple Sclerosis Journal.
🔹Background: AHSCT is a highly effective treatment for MS patients who have a very active disease course despite receiving standard DMTs. However, the optimal timing for offering AHSCT to patients with the “aggressive” MS phenotype, specifically whether it should be used as a first-line treatment, was unknown.
🔹Aim: The objective of this study was to explore the safety and efficacy of AHSCT when used as a first-line DMT in patients diagnosed with ‘aggressive’ multiple sclerosis.
🔹Key Findings:
- Cohort: A total of 20 patients with aggressive MS were retrospectively identified from five international centers.
- Baseline Status: The median time from diagnosis to AHSCT was very short (5 months). All patients had multiple poor prognostic markers, and the median pre-transplant Expanded Disability Status Scale (EDSS) score was 5.0 (range 1.5–9.5), indicating significant disability.
- Efficacy: After a median follow-up of 30 months, the median EDSS score improved significantly to 2.0(p<0.0001).
- Remission: No patient experienced further clinical relapses. After accounting for short-term post-transplant MRI activity, the cumulative NEDA (No Evidence of Disease Activity) rate was 100%.
- Safety: The procedure was deemed safe, with no reported Grade 4 toxicities or treatment-related mortality.
🔹Conclusions: AHSCT is both safe and highly effective when utilized as a first-line DMT for inducing rapid and sustained disease remission and achieving a significant improvement in disability in carefully selected patients with aggressive MS. These findings support considering AHSCT early in the disease course for this specific, highly active phenotype.
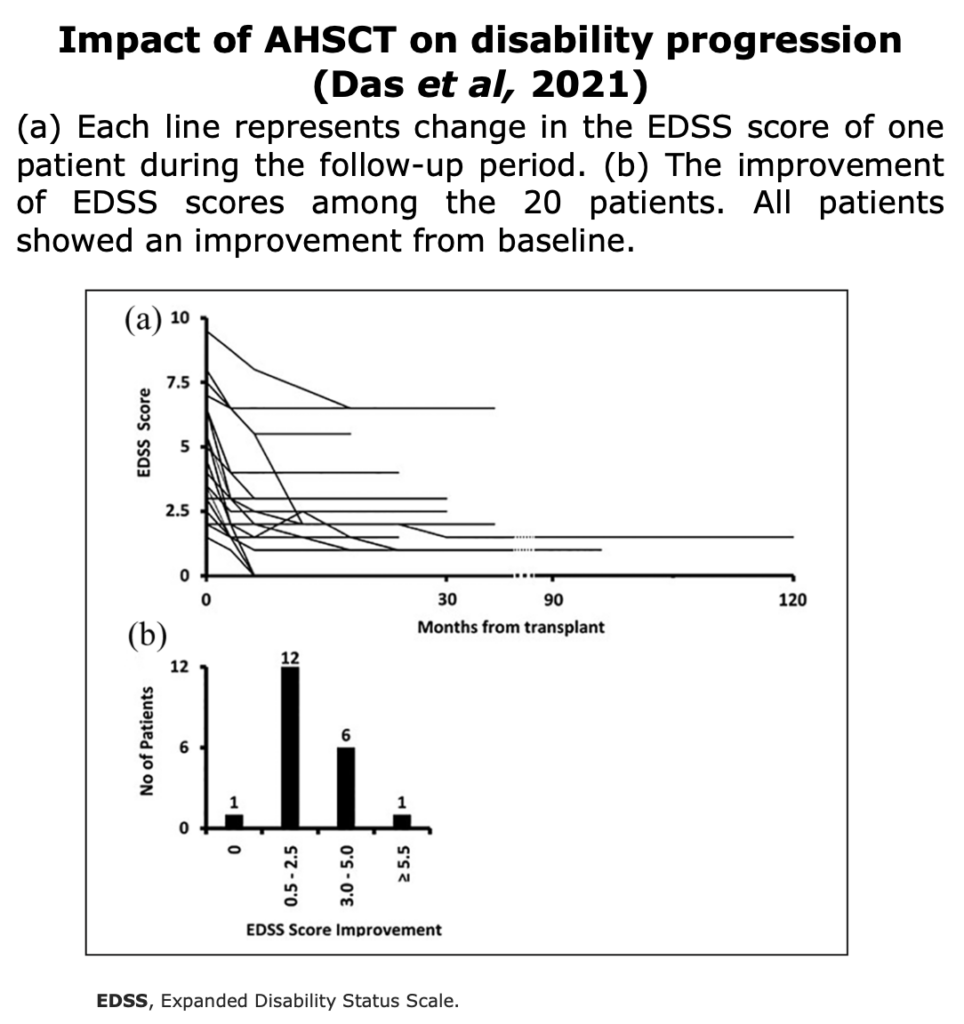
Figures from Das et al. “Autologous haematopoietic stem cell transplantation as a first-line disease- modifying therapy in patients with “aggressive” multiple sclerosis”. Multiple Sclerosis Journal (2021)
Zhukovsky et al., 2021. “Autologous haematopoietic stem cell transplantation compared with alemtuzumab for relapsing–remitting multiple sclerosis: an observational study”. Journal of Neurology, Neurosurgery & Psychiatry.
🔹Background: AHSCT and alemtuzumab (ALZ) are both considered highly efficacious disease-modifying therapies (DMTs) for RRMS. Prior trials had compared AHSCT primarily to less potent DMTs, leaving a gap in real-world evidence comparing AHSCT head-to-head against a highly active agent like ALZ in terms of long-term efficacy and safety.
🔹Aim: The objective was to compare the long-term efficacy and safety outcomes of AHSCT and ALZ in an observational cohort of patients with active RRMS.
🔹Key Findings:
- Efficacy (NEDA-3): The primary outcome, the Kaplan-Meier estimate for NEDA-3 at 3 years, was achieved by 88% of patients treated with AHSCT, compared to 37% of patients treated with ALZ (p<0.0001).
- Relapse Rate: The annualised relapse rate (ARR) was significantly lower after AHSCT (0.04) compared to ALZ (0.1) (p=0.03).
- Disability Improvement: AHSCT resulted in a greater proportion of patients with confirmed disability improvement (57%) and fewer with confirmed disability worsening (1%) at last follow-up, compared to ALZ (45% improved, 12% worsened).
- Early Safety (First 100 days): Adverse events (AEs) of Grade 3 or higher were much more frequent in the AHSCT group (48/69 patients), mainly due to manageable febrile neutropenia. No patients in the ALZ group experienced severe AEs during this period.
- Late Safety (Autoimmunity): Late AEs, particularly autoimmune disorders, were more frequent with ALZ. The risk of developing thyroid disease at 3 years was significantly higher for ALZ (46%) compared to AHSCT (21%)(p=0.005).
🔹Conclusions: In this observational cohort, AHSCT was associated with a higher probability of maintaining NEDA and greater disability improvement than ALZ. While AHSCT has a greater risk of severe, short-term, acute adverse events, ALZ is associated with a significantly higher burden of long-term, autoimmune adverse events. AHSCT may be the preferred choice for patients willing to accept a high short-term risk for a higher probability of long-term, drug-free disease control.
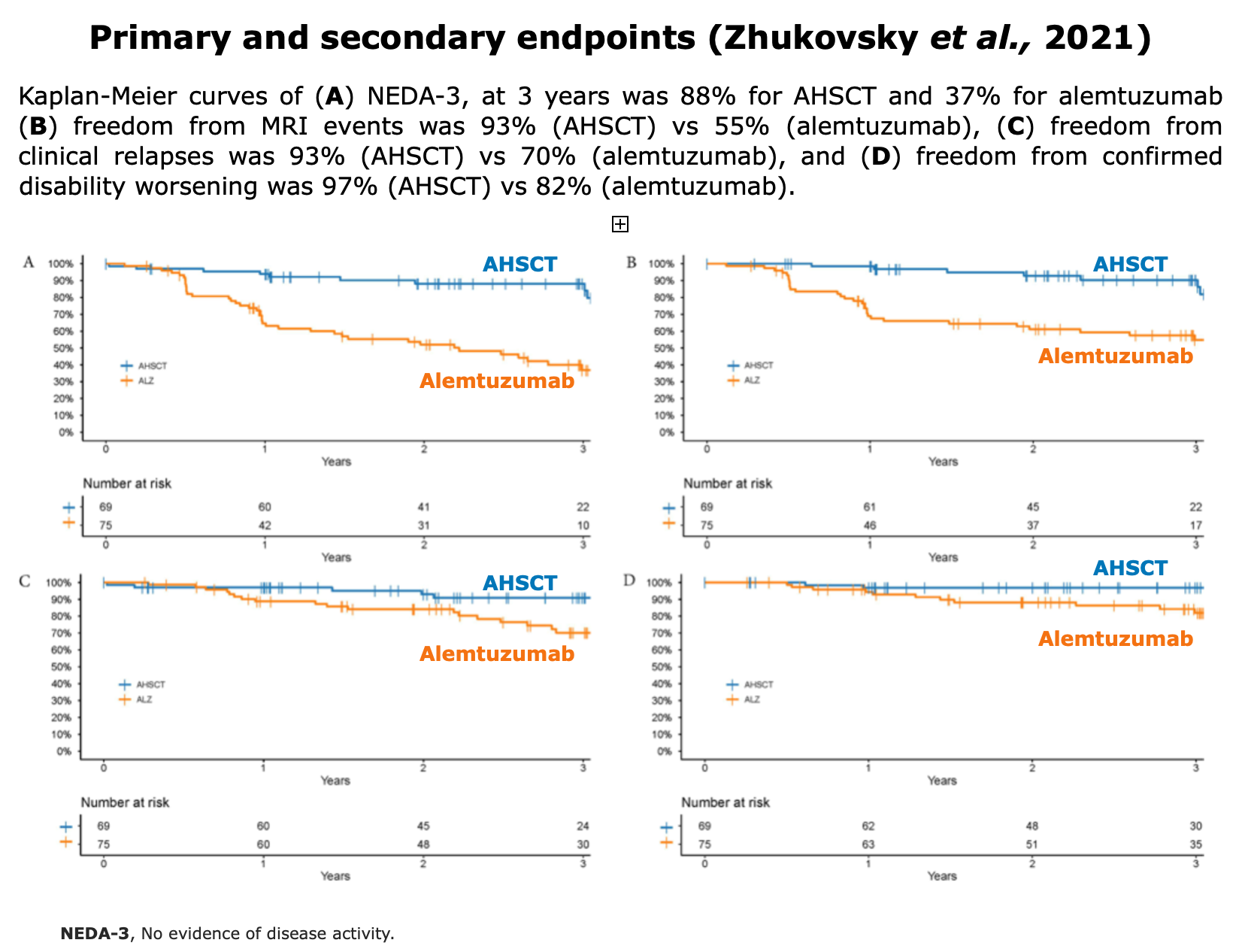
Figures from Zhukovsky et al. “Autologous haematopoietic stem cell transplantation compared with alemtuzumab for relapsing–remitting multiple sclerosis: an observational study”. J Neurol Neurosurg Psychiatry (2021)
Nicholas et al., 2021 “Autologous Hematopoietic Stem Cell Transplantation in Active Multiple Sclerosis. A Real-world Case Series”. Neurology
🔹Background: AHSCT has been shown in clinical studies to profoundly suppress MS activity and induce long-term clinical stabilization. However, data on its effectiveness and safety in a broader, real-world patient population, which often includes people with more severe or progressive disease, was needed.
🔹Aim: To examine the clinical efficacy outcomes and adverse events in a consecutive, real-world cohort of PwMS treated with AHSCT at two major transplant centers in London, UK, to see if real-world outcomes match those reported in highly selective clinical trials.
🔹Key Findings:
- Cohort: The study included 120 PwMS; 52% had progressive MS (Primary or Secondary Progressive MS) and 48% had RRMS. The median baseline disability score (EDSS) was 6.0, and 90% of patients showed MRI activity prior to AHSCT.
- Relapse-Free Survival: MS relapse-free survival was 93% at 2 years and 87% at 4 years overall. Relapses post-AHSCT occurred only in the RRMS subgroup.
- MRI Activity: 90% of participants were free of new MRI lesions at 2 years, and 85% at 4 years.
- Disability: EDSS score progression-free survival (PFS) was 75% at 2 years and 65% at 4 years. The RRMS subgroup showed a small average improvement in EDSS score at 12 months, while the progressive MS subgroup showed further deterioration.
- Predictors: The presence of high monoclonal paraproteinemia was identified as a significant variable associated with worse EDSS score progression-free survival.
- Safety: There were 3 transplantation-related deaths within 100 days (2.5%), all linked to fluid overload and cardiopulmonary complications.
🔹Conclusions: The efficacy outcomes of AHSCT achieved in this real-world cohort, which included a high proportion of patients with progressive MS, are similar to the profound disease suppression reported in more stringently selected clinical trial populations. However, the study suggests that the transplantation-related risks (mortality and morbidity) may be higher in this real-world setting, highlighting the need for careful patient selection and management of complications like fluid overload.
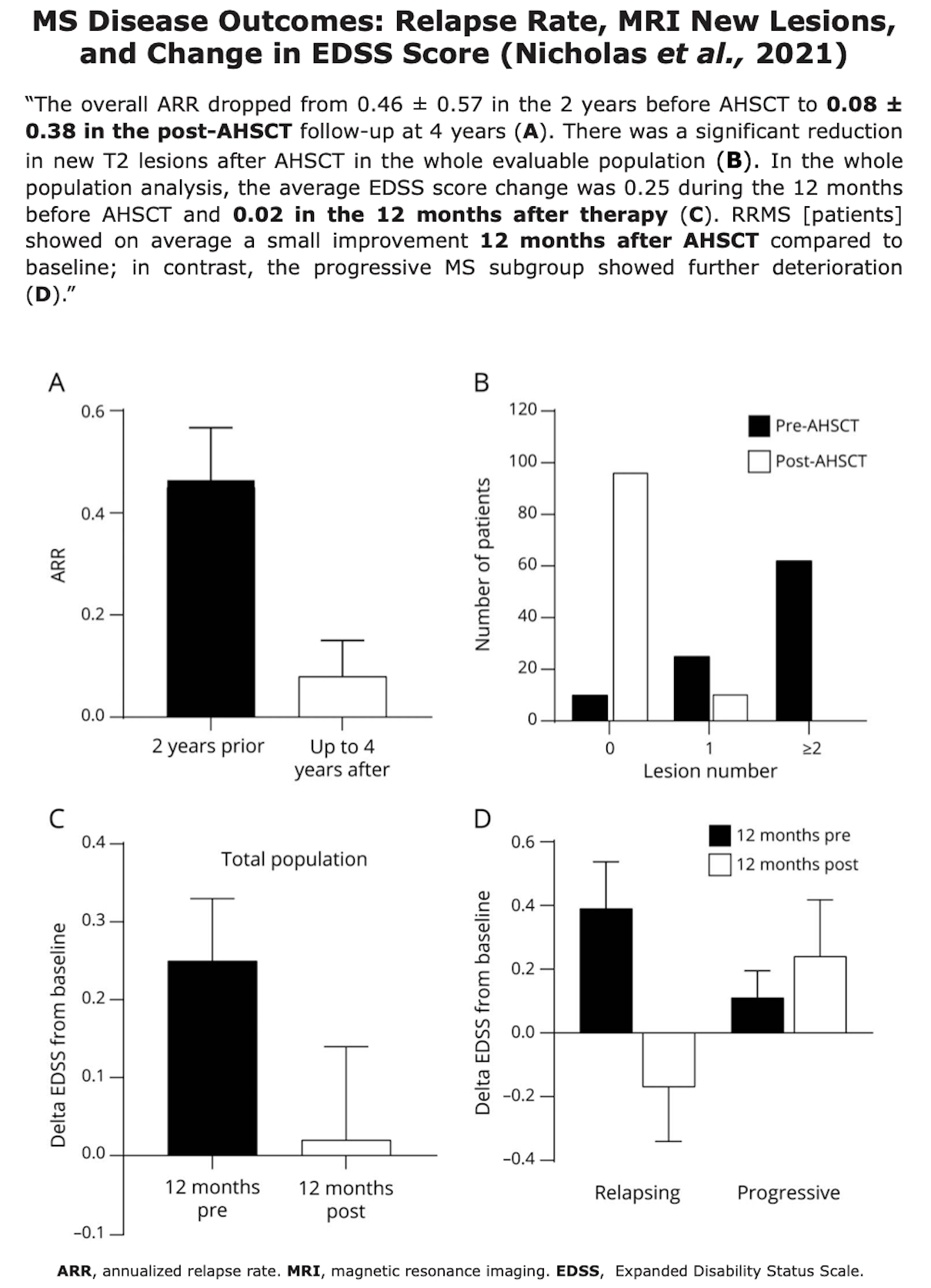
Figure from Nicholas et al., 2021
Boffa et al., 2020 “Aggressive multiple sclerosis: a single-centre, real-world treatment experience with autologous haematopoietic stem cell transplantation and alemtuzumab”. European Journal of Neurology
🔹Background: The ideal treatment for aggressive RRMS is unclear. Both AHSCT and alemtuzumab (ALZ) are potent immune-modulating therapies used for this phenotype. This study sought to provide real-world comparative data on their long-term effectiveness.
🔹Aim: The objective was to compare the efficacy in terms of disease control (NEDA-3) and the safety profiles of AHSCT versus alemtuzumab in a single-center cohort of patients with aggressive RRMS.
🔹Key Findings:
- Cohort: 57 aggressive RRMS patients were included (AHSCT: n=25; ALZ: n=32). The AHSCT group had higher baseline disease activity (higher median EDSS, higher Annualized Relapse Rate, and more MRI lesions).
- Efficacy (NEDA-3): NEDA-3 was achieved by 75% of the AHSCT group compared to 56% of the ALZ group at the end of follow-up.
- Inflammatory Activity: AHSCT showed a significantly greater suppression of inflammation, with a reduced risk of relapse and new MRI activity compared to ALZ (P≤0.012 for both). The ARR at 36 months was much lower with AHSCT (0.05) than with ALZ (0.35).
- Disability: AHSCT demonstrated a significant advantage in promoting EDSS improvement compared to ALZ (P=0.035).
- Safety: Early adverse events (infections/cytopenia) were more frequent with AHSCT. However, late adverse events, particularly autoimmune disorders (e.g., thyroid disease), were significantly more common with ALZ (9 patients) than with AHSCT (1 patient).
🔹Conclusions: While both treatments are effective, AHSCT was superior to alemtuzumab in achieving NEDA-3 status and improving disability in patients with aggressive RRMS, suggesting better long-term suppression of inflammatory activity. The study highlights the trade-off: higher short-term risk with AHSCT versus higher long-term risk of secondary autoimmunity with ALZ.

Figures from Boffa et al. “Aggressive multiple sclerosis: a single-centre, real-world treatment experience with autologous haematopoietic stem cell transplantation and alemtuzumab”. European Journal of Neurology (2020)
🔹Background: AHSCT is a treatment option for aggressive MS that has failed standard therapies. However, most available data were limited to short-term follow-up. Long-term data from a large patient cohort were necessary to assess the long-term course, risks, and complications of MS after AHSCT.
🔹Aim: To evaluate the long-term outcomes in a large multicenter cohort of patients who underwent AHSCT for MS, specifically analyzing progression-free survival (PFS), overall survival, and transplant-related mortality.
🔹Key Findings:
- Cohort and Follow-up: The study included 281 patients from 25 centers with a median follow-up of 6.6 years. The majority of patients (78%) had progressive forms of MS.
- Progression-Free Survival (PFS): The overall probability of MS progression-free survival (PFS) was 46% at 5 years. The PFS rate was significantly higher for the relapsing MS subgroup, reaching 73% at 5 years.
- Overall Survival (OS) and Safety: Overall survival was 93% at 5 years. Transplant-related mortality (TRM), defined as death within 100 days of transplant, was 2.8% (8 deaths).
- Predictors of Better Outcome: Factors significantly associated with better long-term neurological outcomes included younger age, relapsing form of MS, fewer prior disease-modifying therapies, and lower baseline disability.
🔹Conclusions: In this large observational study, AHSCT was effective, with nearly half of the patients remaining free from neurological progression for 5 years. The procedure offers a clear benefit, particularly for patients with the relapsing form of MS. The findings underscore the importance of early intervention and careful patient selection to maximize the long-term benefit of AHSCT.
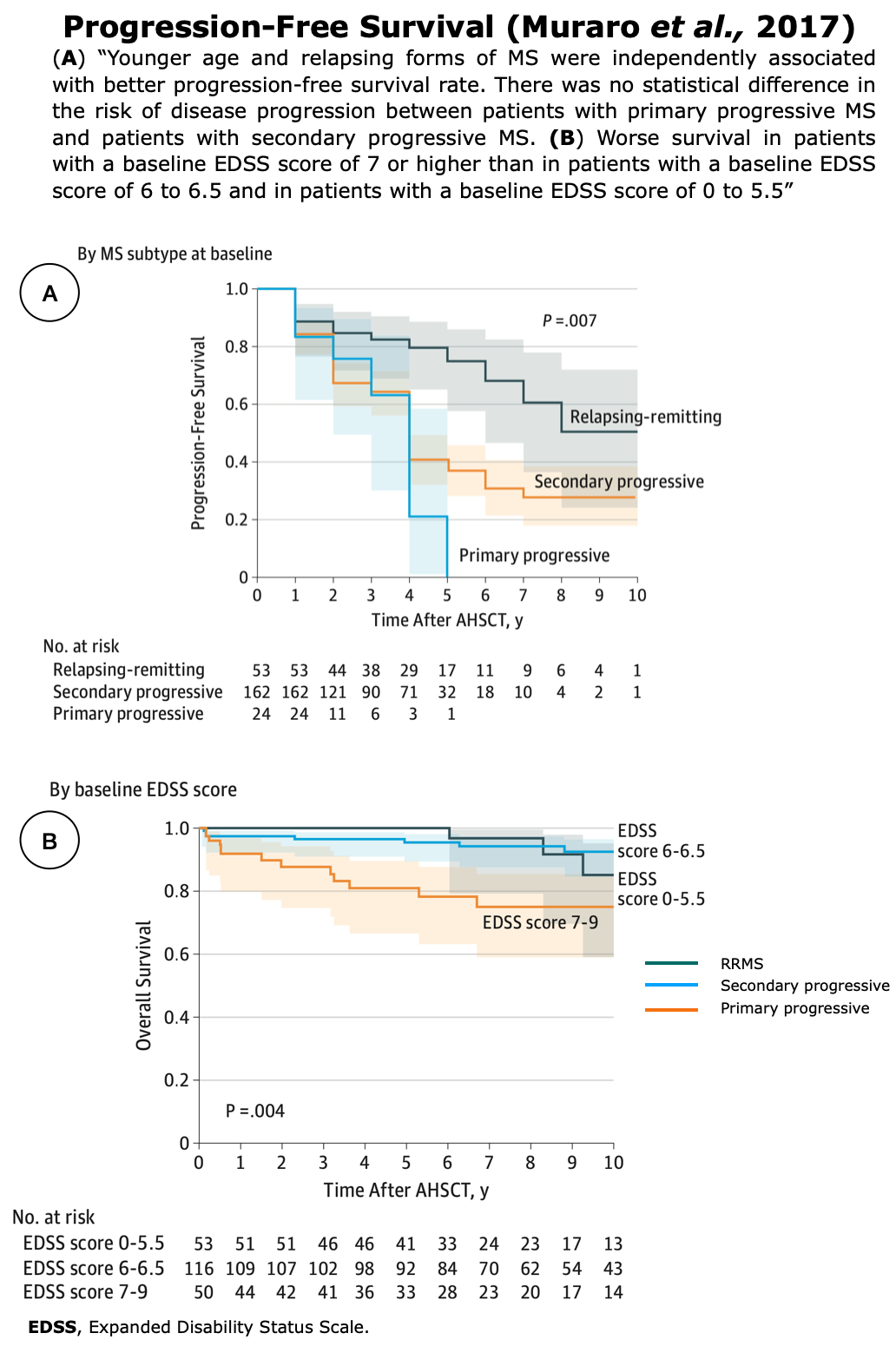
Figures from Muraro et al. “Long-term Outcomes After Autologous Hematopoietic Stem Cell Transplantation for Multiple Sclerosis”. JAMA Neurology (2017)
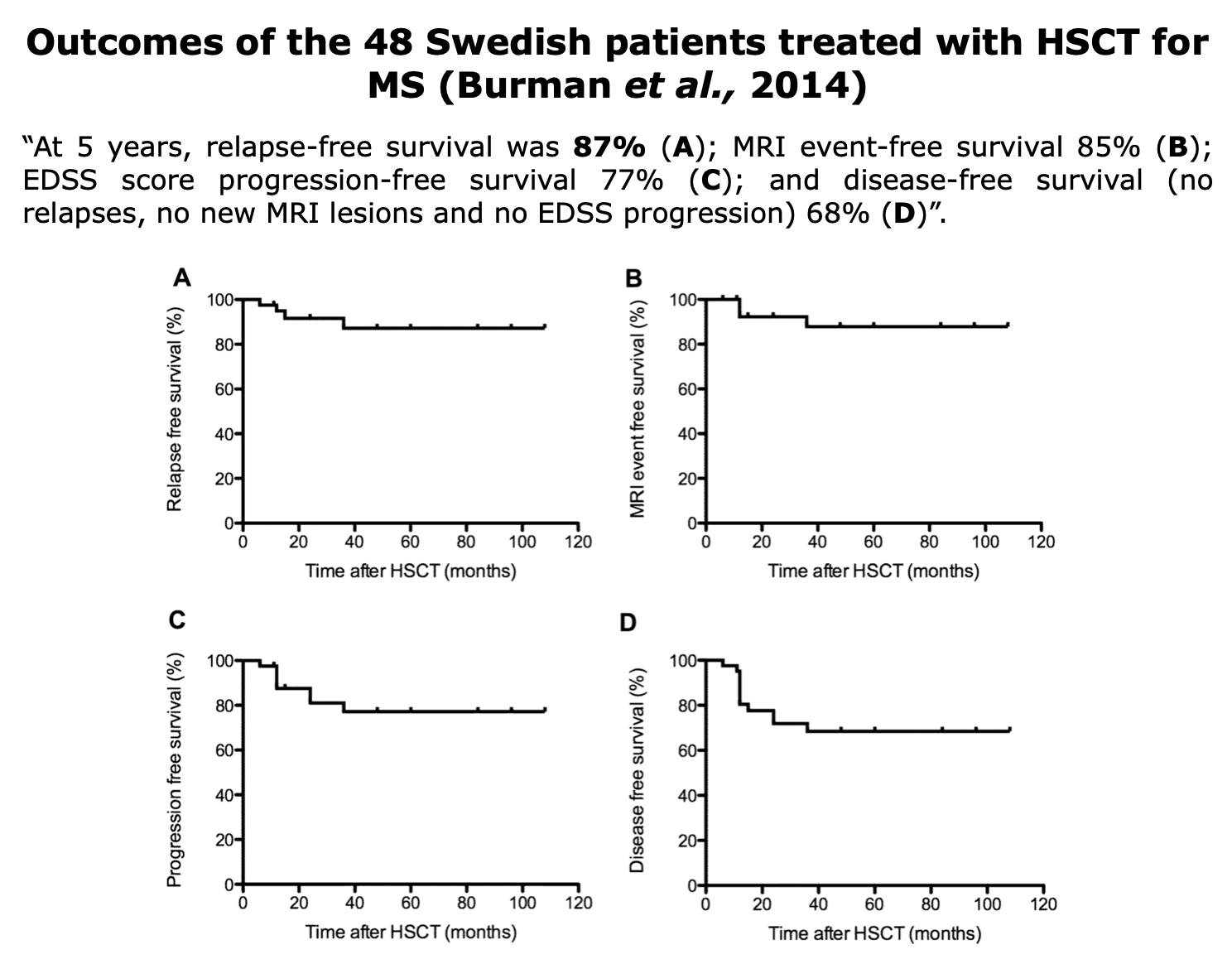
Burman et al.,2014. “Autologous haematopoietic stem cell transplantation for aggressive multiple sclerosis: the Swedish experience“. Journal of Neurology, Neurosurgery & Psychiatry.
🔹Background: AHSCT is considered a viable treatment option for aggressive MS. Since no randomized controlled trials had been performed, systematic and sustained follow-up data were crucial to assess the safety and long-term efficacy of this procedure in a real-world setting.
🔹Aim: The objective was to describe the characteristics and outcome of all consecutive Swedish patients treated with HSCT for aggressive MS to provide important information on the treatment’s safety and efficacy.
🔹Key Findings:
- Cohort and Follow-up: The study included 48 patients evaluated for safety, with 41 patients having at least 1 year of follow-up (mean follow-up: 47 months). Most patients (83%) had relapsing-remitting MS (RRMS), and the median EDSS score at the decision for HSCT was 6.0.
- Efficacy at 5 Years:
- Relapse-free survival was 87%.
- MRI event-free survival was 85%.
- EDSS score progression-free survival was 77%.
- Disease-free survival (NEDA-3) was 68%.
- Disability Improvement: The median EDSS score for RRMS patients improved from 5.5 at HSCT to 3.0 at 2 years. The median change in EDSS for RRMS patients was -1.5.
- Prognostic Factor: The presence of gadolinium-enhancing (Gd+) lesions prior to HSCT was associated with a favorable outcome, resulting in a significantly higher disease-free survival rate (79% vs 46%; p=0.028).
- Safety: There was no treatment-related mortality (TRM) recorded. The most common long-term side effects were herpes zoster reactivation (17%) and thyroid disease (8.3%).
🔹Conclusions: AHSCT with a low-to-intermediate intensity protocol is a highly effective treatment for inflammatory active MS, leading to long-term disease remission in the majority of patients. It can be performed with a high degree of safety at experienced centers. The study supports the principle that patients with evidence of active inflammation at baseline are the most likely to benefit.
Case-Series
Expert Opinion
Sormani et al. (2017, MSJ) argue that AHSCT reaches NEDA far more reliably than any DMT (78–83% at 2 years, 60–68% at 5 years) despite treating more aggressive patients, with TRM down to ~1.3%. Conclusion: a phase 3 RCT is warranted to formally establish AHSCT’s risk/benefit profile.
Sormani et al. “NEDA status in highly active MS can be more easily obtained with autologous hematopoietic stem cell transplantation than other drugs”. Multiple Sclerosis Journal.
🔹Background: NEDA—absence of relapses, disability progression, and MRI activity—is an emerging therapeutic goal in RRMS. With current DMTs, only 13–46% of patients reach NEDA after 2 years, and maintenance over time is uncommon.
🔹Aim: To assess how effectively AHSCT achieves NEDA compared with DMTs in highly active RRMS.
🔹Key Findings:
- AHSCT induces an “immune reset” that can more effectively suppress disease activity.
- In clinical studies, 78–83% of AHSCT-treated patients maintained NEDA at 2 years and 60–68% at 5 years—significantly higher than with any approved DMT.
- This advantage is notable because AHSCT patients generally have more aggressive disease than those enrolled in DMT trials.
- Transplant-related mortality has markedly decreased to ~1.3% since 2001, with no deaths reported in recent RRMS cohorts.
- Nonmyeloablative conditioning regimens improve safety while preserving efficacy.
🔹Conclusions: AHSCT yields markedly higher and sustained NEDA rates than DMTs, with improved safety. A phase 3 randomized trial is warranted to confirm its efficacy and risk–benefit profile, potentially establishing aHSCT as a cost-effective therapy for highly active MS.
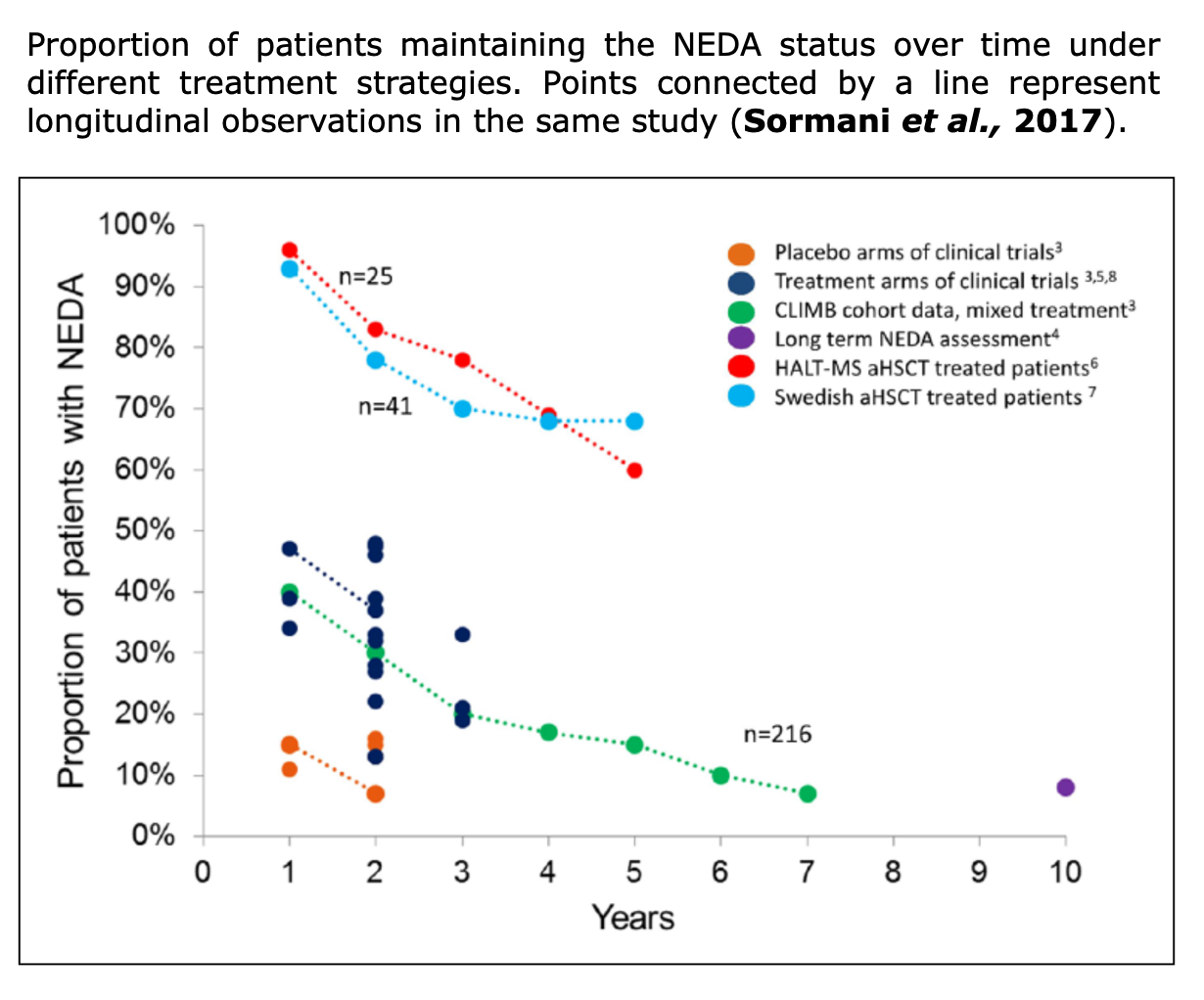
Figure from Sormani et al. “NEDA status in highly active MS can be more easily obtained with autologous hematopoietic stem cell transplantation than other drugs”. Multiple Sclerosis Journal (2017).
Immunological Evidences
Understanding Immune Reconstitution After AHSCT for MS
When you undergo AHSCT for MS, your immune system goes through a complete “reset.” Here’s how it works in simple terms:
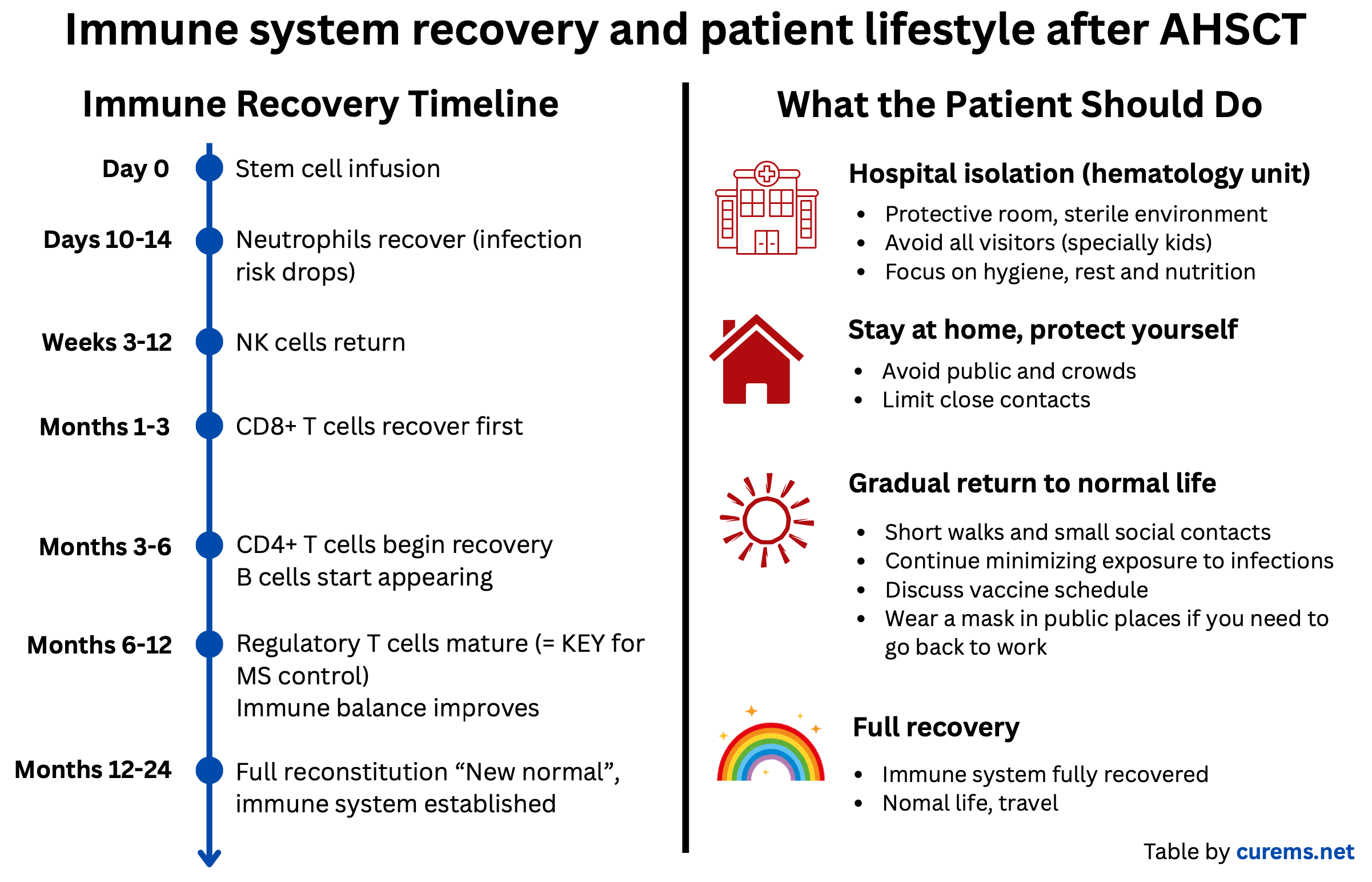
Following the immune reconstitution timeline from day 0 to full recovery:
1. The Reset Phase (Day 0 – 2 weeks)
2. The Rebuilding Phase (Weeks to 12 Months)
3. Full Recovery (12–24 months)
By this stage, most people reach a “new normal”, where the immune system functions well and infection risk is low. Immune balance and tolerance are re-established.
-
Different types of T and B cells regain their normal numbers and function.
-
The immune system becomes capable of responding to new infections and vaccines.
-
Regulatory T cells help maintain long-term tolerance, keeping autoimmune activity under control.
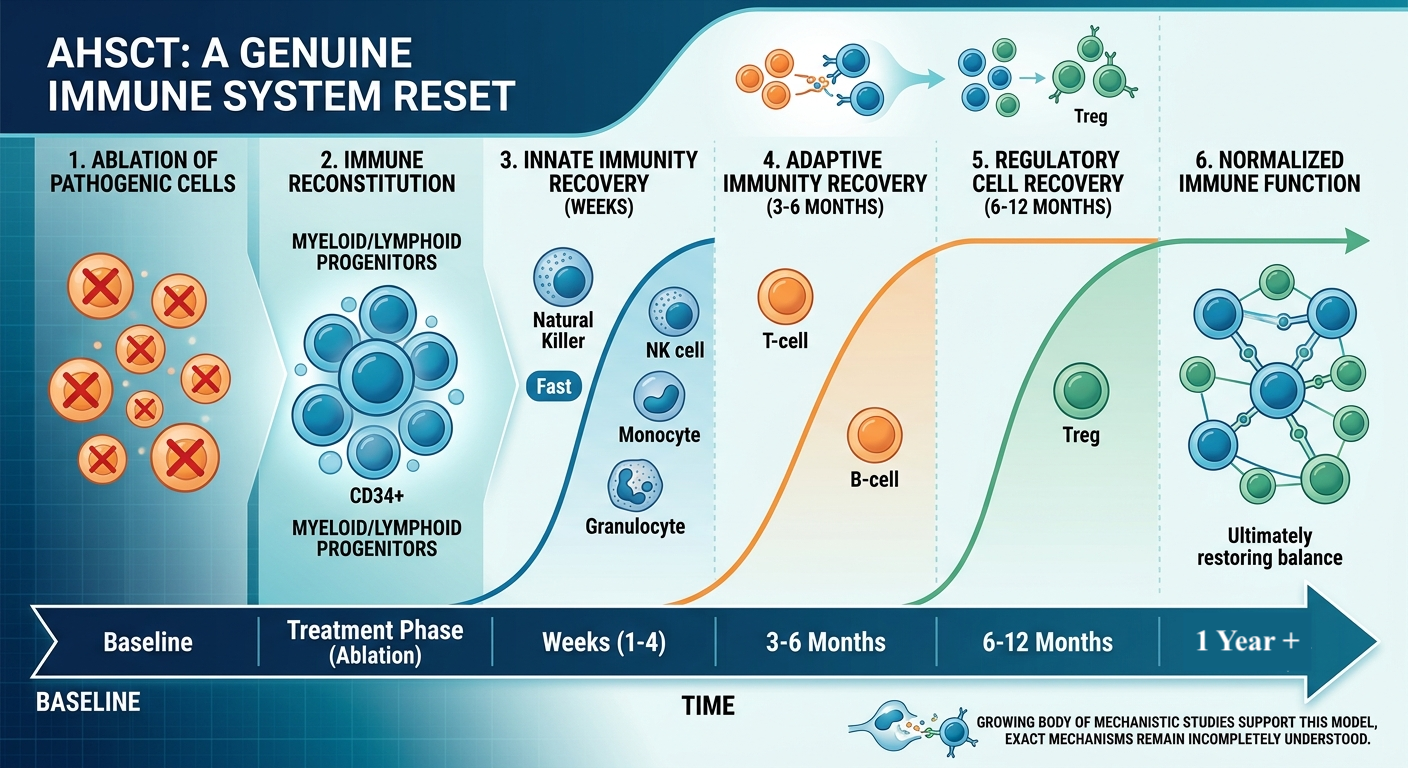
Immune reconstitution post-AHSCT. Figure by curems.net (modified with Gemini)
Papers on IR
IR, Immune Reconstitution Post-AHSCT
Across immunological studies, AHSCT consistently shows deep depletion of autoreactive/pro-inflammatory populations, a shift toward naïve, tolerogenic immune profiles, and biomarker changes (CSF, MRI, miRNA) that track with durable clinical remission — reinforcing the “immune reset” model, though the precise causal mechanisms are still being mapped out.
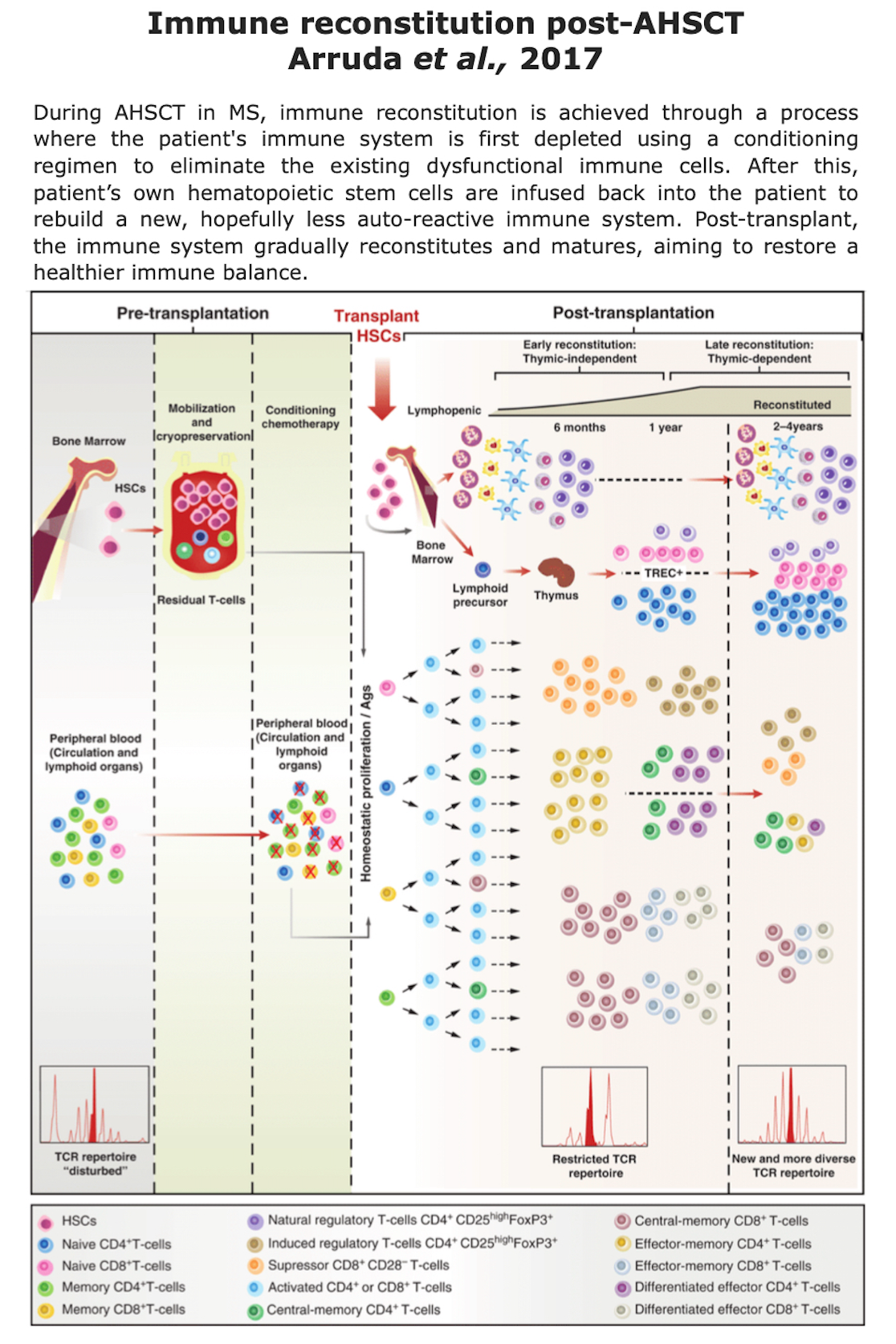
✅ 0–3 months — early adaptive reconstitution (Ruder et al., 2022; von Niederhäusern et al., 2022; Mariottini et al., 2024): Naïve T cells are nearly absent immediately post-transplant, while effector memory CD4+ T cells reconstitute rapidly (though with shorter telomeres and senescence markers). Total B-cell numbers recover by 3 months. Thymic hyperplasia — radiological evidence of de novo thymopoiesis — has been detected as early as 1–3 months post-AHSCT in a subset of patients.
✅ Sustained remodeling confirmed at 24 months (Gavasso et al., 2025; Müller et al., 2025): High-dimensional (mass cytometry) profiling confirms profound, sustained remodeling of innate and adaptive immunity over 24 months, including long-term depletion of pro-inflammatory CD161+ T cells and Th1/Th17 subsets, and a durable shift toward naïve B cells. Higher pre-transplant switched memory B-cell levels predicted post-AHSCT disease activity.
Marchi et al., 2024 “Leptomeningeal enhancement in multiple sclerosis: a focus on patients treated with hematopoietic stem cell transplantation”. Front. Neurol. Sec. Multiple Sclerosis and Neuroimmunology.
Background: Leptomeningeal enhancement (LME) is a nonspecific MRI finding seen in various neurological diseases, including MS, and is linked to worse outcomes. It may reflect localized, compartmentalized immune activity in the CNS and is being explored as a biomarker of disease severity.
Aim: To assess the impact of AHSCT on LME in MS, using a BEAM+ATG regimen.
Key Findings:
-
In one patient, an LME focus disappeared after AHSCT, suggesting potential disruption of CNS-compartmentalized inflammation.
-
A correlation was found between the number of LMEs and age at AHSCT, not age at MRI.
-
The results support the hypothesis that early, high-efficacy, CNS-penetrant therapies might reduce leptomeningeal inflammatory aggregates (e.g., ELFs) and limit inflammation compartmentalization.
Conclusions: AHSCT may halt or reverse LME in MS. Further long-term, prospective studies are needed to determine if LME can serve as a treatment response marker for therapies acting within the CNS.
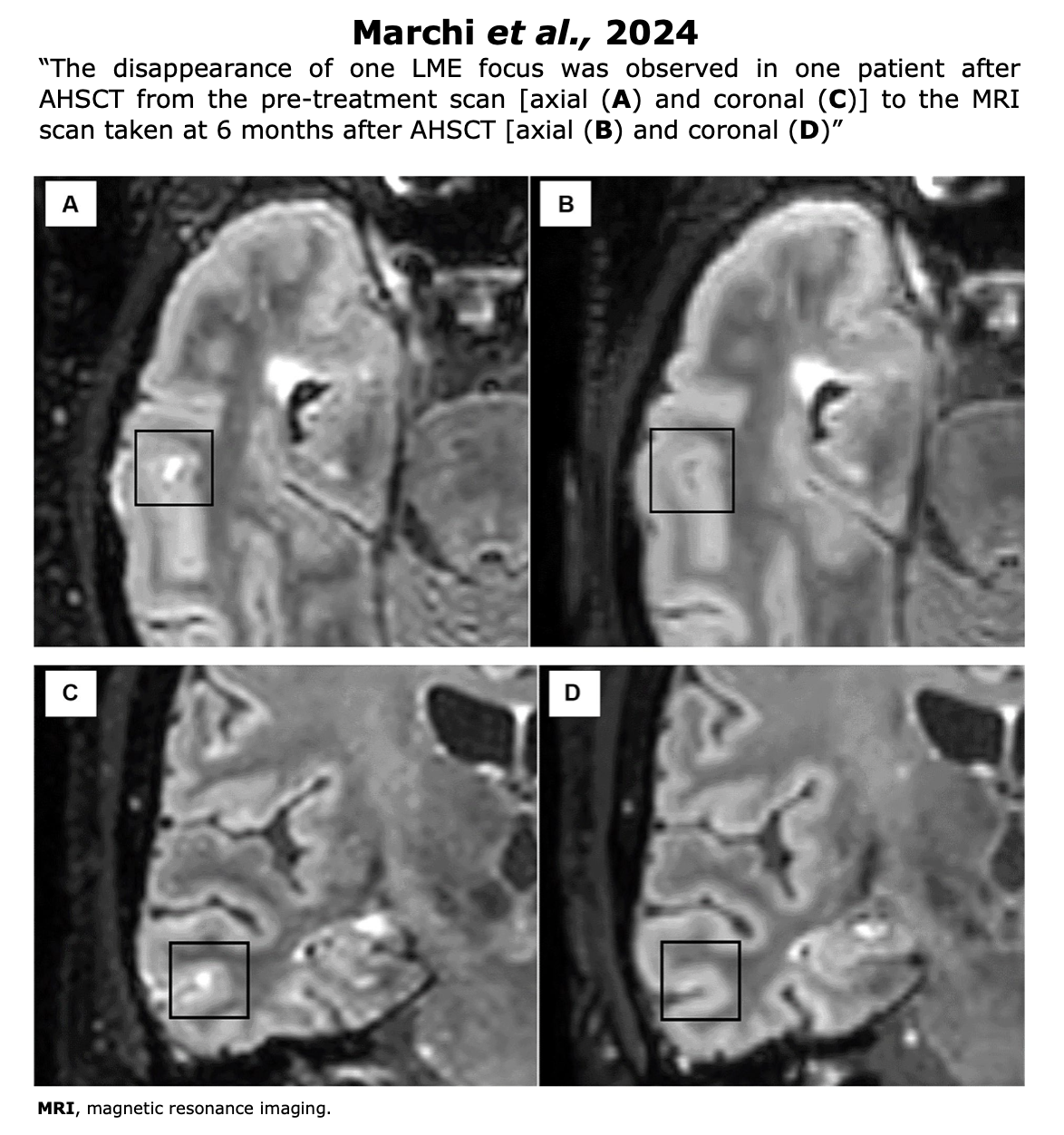
Figure from Marchi et al. “Leptomeningeal enhancement in multiple sclerosis: a focus on patients treated with hematopoietic stem cell transplantation”. (2024) Front. Neurol. Sec. Multiple Sclerosis and Neuroimmunology.
Burt et al. “New autoimmune diseases after autologous hematopoietic stem cell transplantation for multiple sclerosis”. Bone Marrow Transplantation
A part of this paper is dedicated to IR.
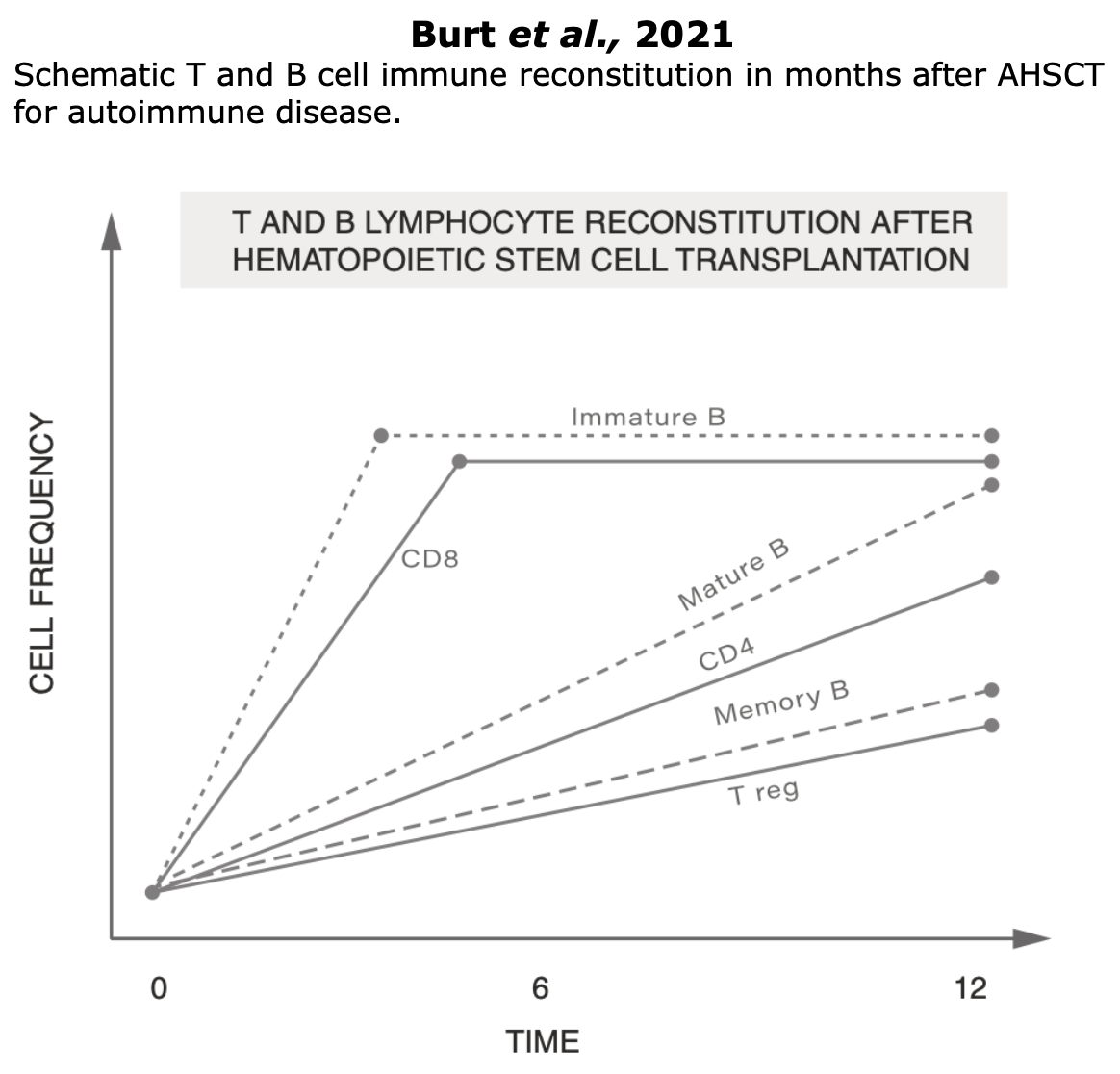
Figure Burt et al.“New autoimmune diseases after autologous hematopoietic stem cell transplantation for multiple sclerosis”. Bone Marrow Transplantation
Long-Term Benefits
The ECTRIMS/EBMT consensus statement (Muraro et al., 2025) posits that AHSCT should be presented as a therapeutic option to patients with RRMS who fail HE-DMTs.
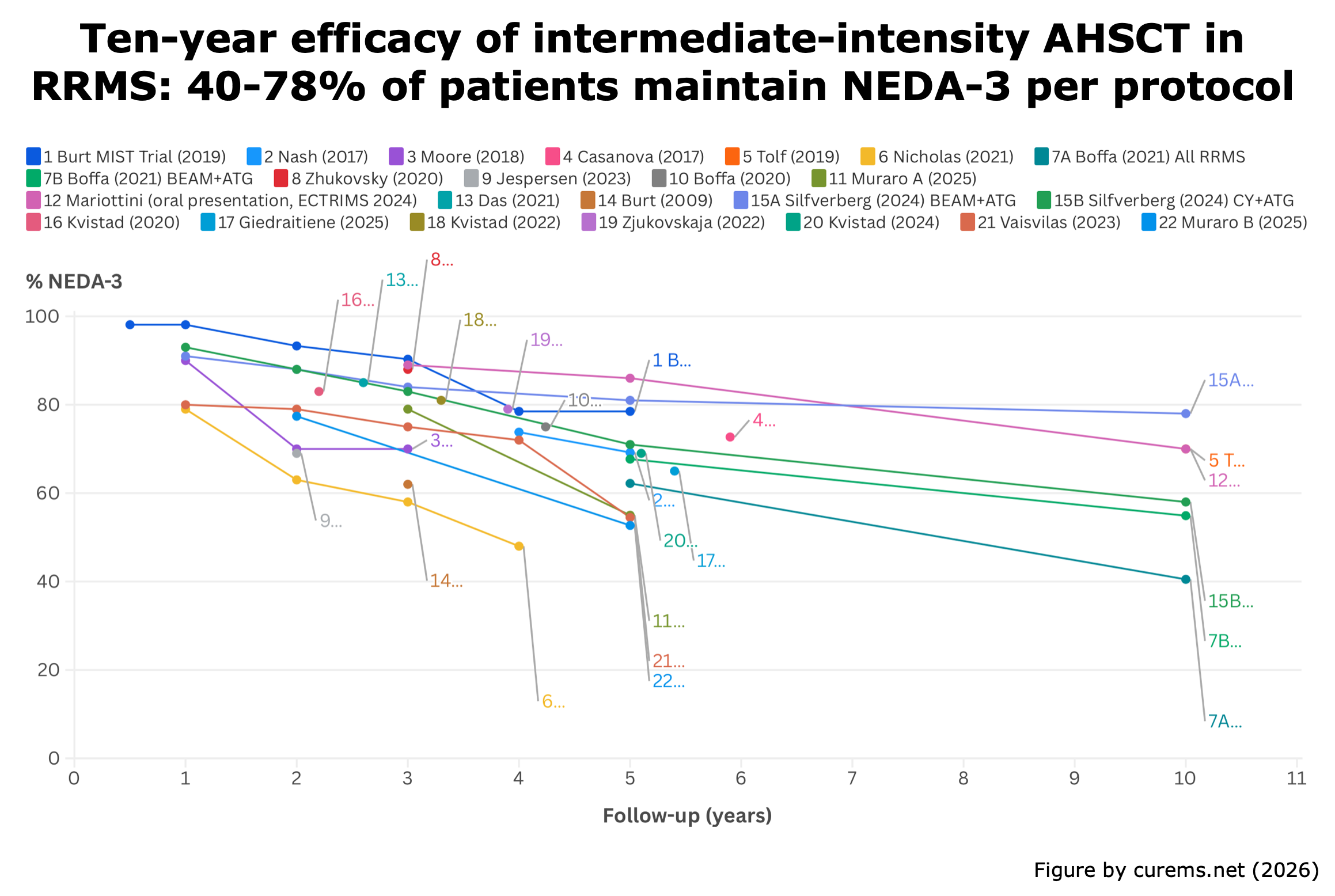
In evaluating the risk/benefit profile of HE-DMTs and AHSCT, neurologists and patients must also consider the unique long-term benefits of AHSCT. Notably, over 50% of RRMS achieve NEDA-3 for more than 10 years without requiring further DMT.
In this section, we focus on the long-term benefits of AHSCT, defining “long-term” as the period beyond 1-year post-AHSCT:
An infographic by CureMS.net (2025) illustrating the long-term benefits.
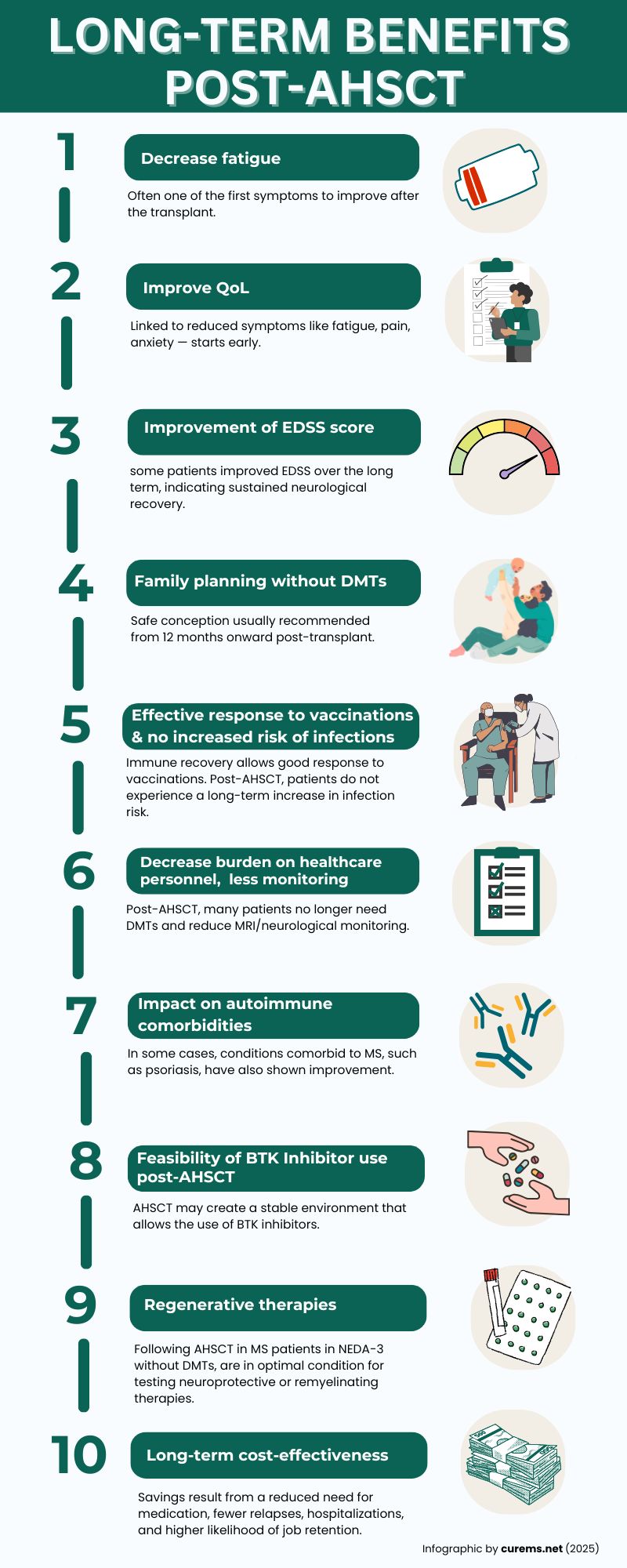
AHSCT, by halting the aberrant immune activity that drives ongoing CNS inflammation, has the potential to directly address one of the primary biological mechanisms underlying fatigue in MS.
Studies have begun to specifically investigate the impact of AHSCT on fatigue (Giedratiene et al., 2022 | Mariottini et al., 2023 | Volz et al., 2024), with emerging evidence suggesting a clinically meaningful improvement in this symptom, particularly in patients with highly active inflammatory disease.
These findings support the hypothesis that durable suppression of CNS inflammation through AHSCT may not only stabilize disability progression but also alleviate one of the most burdensome symptoms of the disease, significantly enhancing patients’ QoL.
Clinical evidence shows marked improvements in physical abilities, energy levels, and symptom relief, which contribute to better emotional health, greater autonomy, and improved social and professional engagement. More about QoL here.
While MS does not impair fertility or pregnancy outcomes, DMTs can complicate family planning, as some are contraindicated during pregnancy and breastfeeding. AHSCT offers a treatment option that allows patients to plan future pregnancies without the ongoing influence of DMTs.
The chemotherapy used in AHSCT may affect fertility; this risk is now routinely addressed through pre-treatment fertility preservation strategies for females such as mature oocyte cryopreservation, embryo cryopreservation or ovarian tissue cryopreservation or sperm cryopreservation for males (Mikulska et al., 2024 – Handbook of Clinical Neurology). See the fertility section here.
There is not an official guideline specifying an exact timeframe for conception after AHSCT; however, clinical observations suggest that pregnancy can generally be considered safe from 12- and 24-months post-transplant, once the immune system has recovered and there is no longer interference from immunosuppressive therapies.
Fertility counseling and early consultation with specialists are strongly recommended before initiating the procedure.
“Published guidance recommends that people who have undergone HSCT are considered as ‘never vaccinated’ and offered revaccination. Vaccination planning after AHSCT should follow national and international recommendations and be adapted to local practice.” (Muraro et al., 2025 | EBMT-ECTRIMS Consensus Statement).
After the first year post-transplant, patients can receive future vaccinations with flexible timing, based on clinical need and patient preference. unlike with DMTs (for vaccination in patients on DMTs see Otero-Romero, et al., 2023 – ECTRIMS/EAN consensus on vaccination).
After 1–2 years post-transplant, the immune system has reconstituted, and the revaccination program is complete. At this point, there is no evidence of an increased risk of infection, and the risk is presumably comparable to the pre-transplant period, whereas the continuous administration of DMTs increases the risk of infection (Langer-Gould et al., 2023 | Moiola et al., 2021)
Immunological and Infectious monitoring following transplant: 
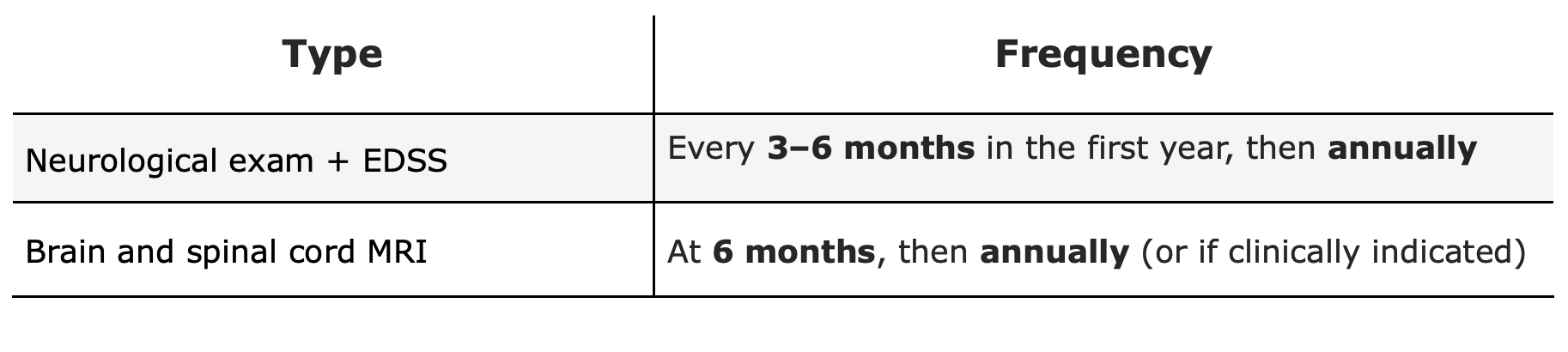
Neurological and Radiological monitoring following transplant:
The use of BTK inhibitors in patients who underwent transplantation one year ago and are not using a DMT may therefore be safer.
Following AHSCT MS patients in NEDA-3 without DMTs, are in optimal condition for testing neuroprotective strategies, such as Neural Stem Cells (Genchi et al, 2023) or NURR1 activators (Fox et al., 2024) or remyelinating therapies such as Lucid-31-302 (phase I trial, read more here), PIPE-307 (see more here) or dihydroartemisinin (link here).
Unlike DMTs, which require lifelong administration, AHSCT is a one-time treatment. This results in substantially lower long-term costs for national healthcare systems, insurance providers, and patients—especially in self-funded cases (for “AHSCT centers & costs”, click here).
As outlined in the “Pharmacoeconomics section” (more here), AHSCT has shown superior cost-effectiveness compared to all available DMTs, whose cumulative and annually increasing costs continue to place a financial burden on healthcare budgets. Worth reading: Santoro et al., 2024 (An American Academy of Neurology Position Statement)
Quality Of Life
WHO defines Quality of Life (QoL) as “an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns”.
In pwMS, QoL is affected in numerous ways and aspects, including their ability to work, perform daily activities, and execute everyday tasks (Rezapour et al., 2017).
Initially, only the physical disability caused due to MS was considered by clinicians, as the sole aspect of the disease. In order to obtain an overview on how MS impairs patients’ QoL both psychological aspects and physical aspects must be considered.
QoL according to FDA: a patient-report outcome
QoL can be considered as a patient-reported outcome (PRO). PROs are defined by the US FDA as the “measurement of any aspect of a patient’s health status that comes directly from the patient, without the interpretation of the patient’s response by a clinician or anyone else” (US Food and Drug Administration 2009) (EBMT handbook – Barata et al., 2024). Consequently, PROs describe the impact that AHSCT has on patients’ lives.
Pharmacoeconomics
Pharmacoeconomics is a specialized branch of economics that assesses the cost and value of pharmaceutical products and services. It examines their cost and the benefits they provide in terms of reducing disease progression, disability, and improving patients’ quality of life (QoL).
Pharmacoeconomics employs various methods, such as cost-effectiveness analysis, to evaluate these aspects. These studies are essential for all healthcare systems, given the increasing challenges in providing medications to all citizens.
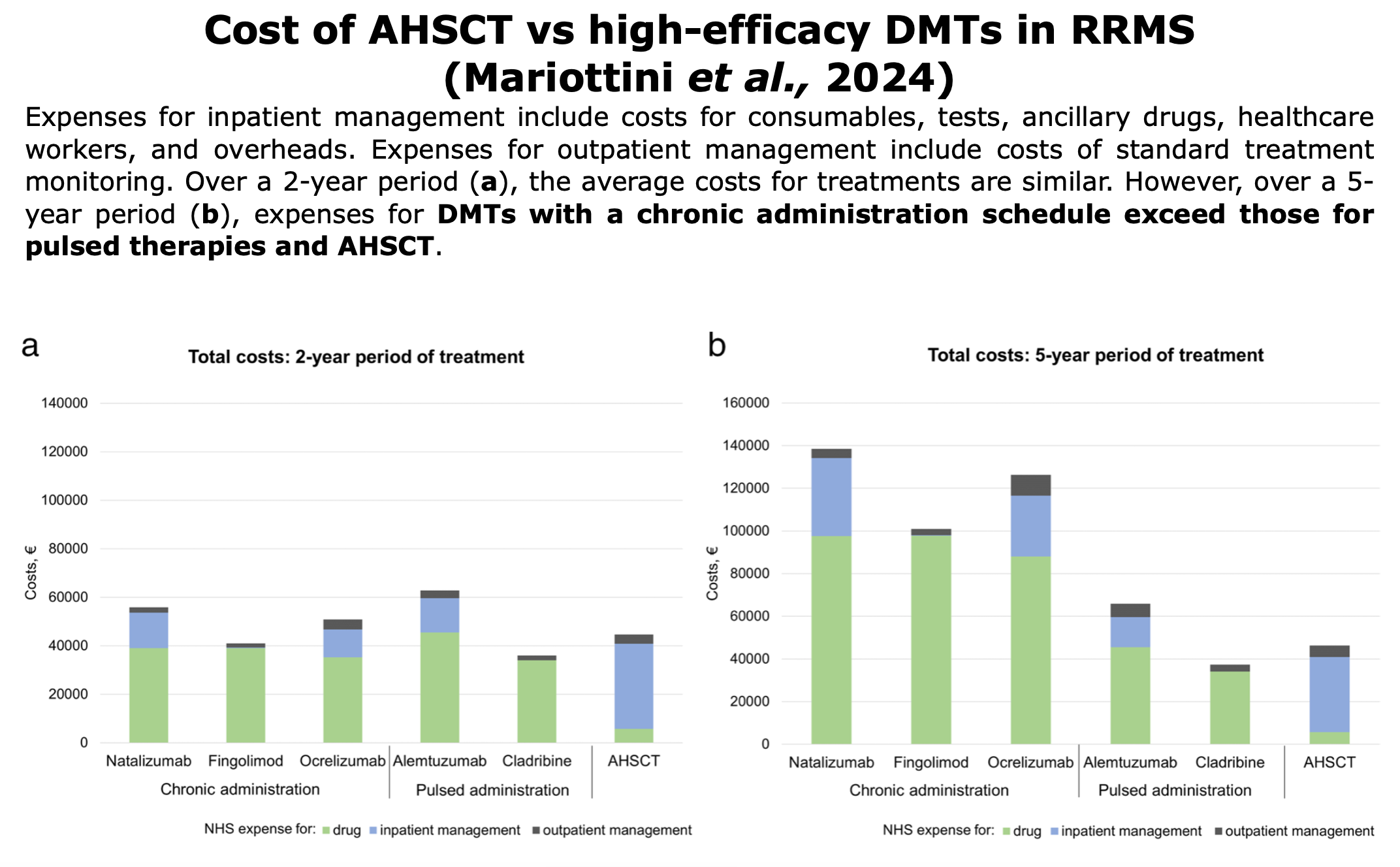
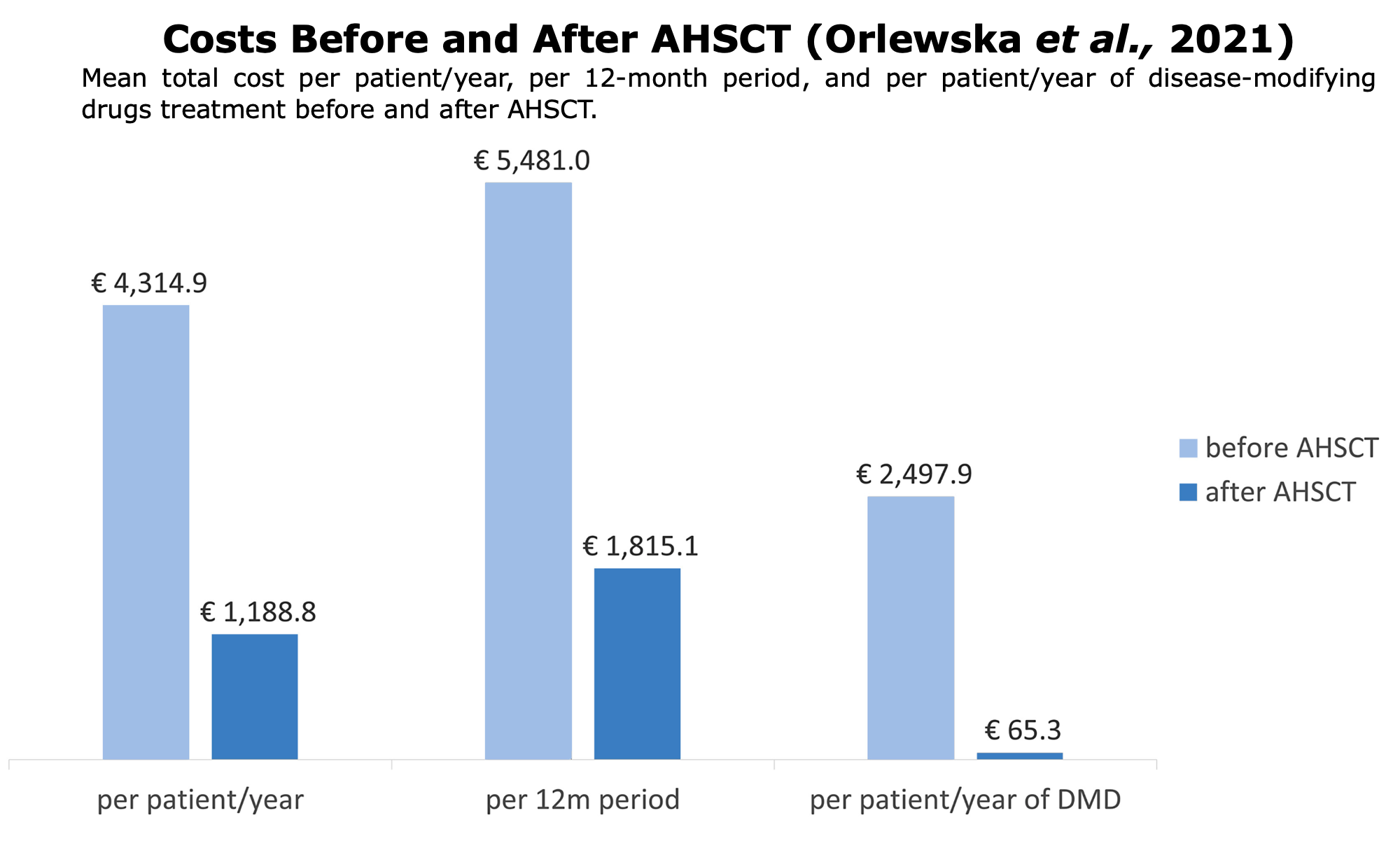
Following studies or reports on pharmacoeconomic around the world comparing AHSCT vs. DMTs:
Tools to Understand Studies
Tools to Understand
Studies
Clinical evidences are information and data collected through scientific studies and clinical observations that demonstrate the efficacy, safety, and effectiveness of treatments or procedures.
To obtain clinical evidences, various types of studies are conducted (e.g., randomized controlled trials, cohort studies, case-control studies, etc.). Each of these studies provides evidence of different strengths.
Click on these links for additional informational about how clinical evidences are collected, phases of clinical trials or class of evidences (Source: Neurology).