Factors Influencing Risks
AHSCT is a one-off treatment and a multistep procedure aimed at resetting the immune system. Like all procedures, drugs, or therapies, AHSCT presents both benefits and associated side effects and risks.
Below, we list three factors that may influence AHSCT outcomes:
AHSCT-related adverse events (i.e., complications) are divided into:
🟢 Early adverse events from the first day of mobilization to 100 days after transplant
🟢 Transplant-related mortality (TRM) within 100 days following transplant
🟢 Late adverse events starting from day 101 after transplant
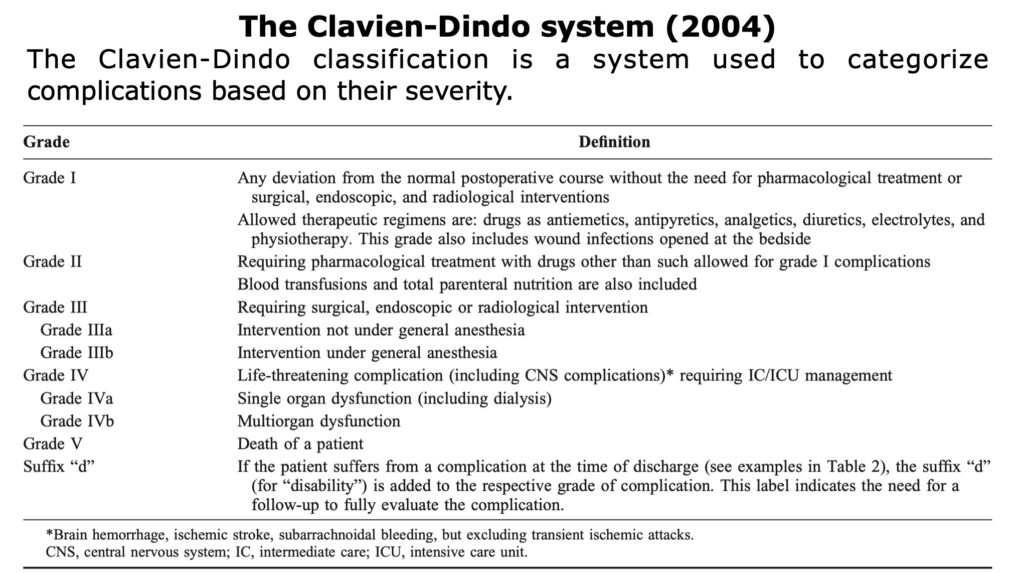
The classification of adverse events was developed by Clavien et al., in 2004, read here the publication or read the insights (blue button).
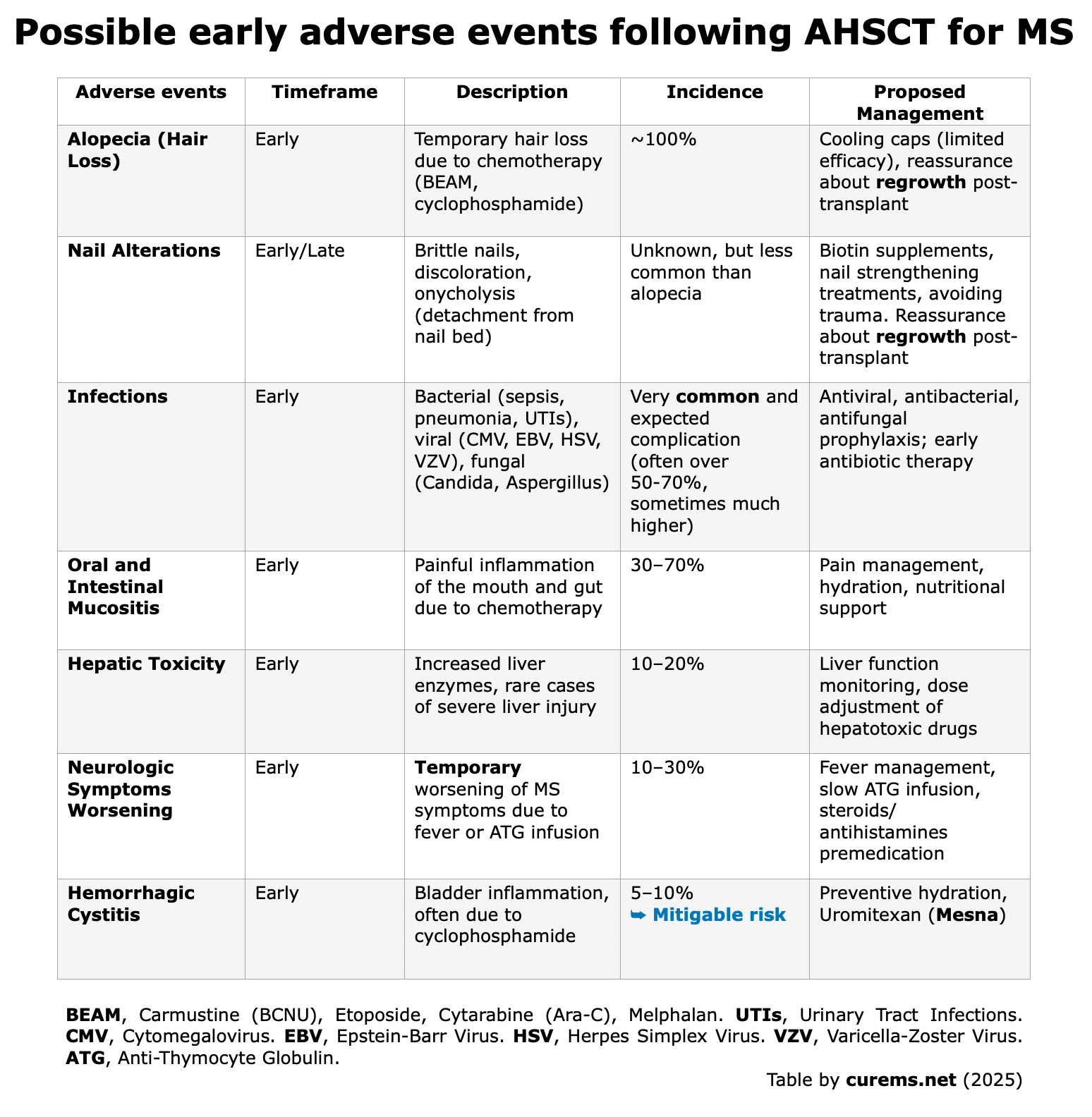
Early Adverse Events
From Mobilization Day 1
to Day 100 Post-AHSCT
The adverse events are caused by the toxicity of the drugs used in mobilization and conditioning regimens. (Atkins et al., 2017)(Bose et al., 2021).
Adverse events are also influenced by the patient’s condition and the DMTs administered prior to AHSCT.
Data obtained from “Hematopoietic Stem Cell Transplantation for Neurologic Diseases“. Chapters 8-10. Handbook of Clinical Neurology (Elsevier, 2024). Edited by Professors M. Inglese and G.L. Mancardi
Common Adverse Events That May Occur During Mobilization:
- Hair loss (alopecia): Hair loss is a temporary adverse event of AHSCT, the hair will regrow within 1 to 6 months. In Jespersen et al. (2023): “All patients [32 patients] developed alopecia during mobilization.”
- Other common AEs include nausea, bone pain (in about 50% of cases), and fatigue (Nicholas et al., 2021) (Jespersen et al., 2023).
Common Adverse Events Related to Conditioning:
- Febrile neutropenia: In this phase, the primary immediate concern is febrile neutropenia, where a low white blood cell count causes high fever, making patients vulnerable to bacterial infections. In some cases, these can be severe.
-
Infections: Early adverse events include bacterial infections and reactivation of latent viral, particularly during the conditioning phase. Notably:
– EBV reactivation may lead to the rare but serious PTLD (an uncontrolled proliferation of B-cells that mimics lymphoma, characterized by fever, weight loss, and lymphadenopathy). To our knowledge, a single fatal case has been reported in a patient treated with high-intensity conditioning (TBI) (Nash et al., 2003). In another study involving 36 patients treated with intermediate conditioning regimen (Mehra et al., 2017), 3 showed imaging findings consistent with PTLD on CT scan, although none had histological confirmation. Additionally, three other MS patients experienced worsening neurological symptoms, one of whom presented with a pseudo-relapse. All six patients were treated with anti-CD20 monoclonal antibody therapy (Rituximab; 375 mg/m² weekly for four weeks), resulting in rapid symptom resolution.
These findings underscore the need for careful monitoring of EBV reactivation in this population and suggest that Rituximab should be considered in selected cases. PCR-based monitoring for EBV is mandatory during the first 100 days (Sharrack et al., 2020).
– CMV can also reactivate, causing organ damage. According to the EBMT-ECTRIMS Consensus Statement (Muraro et al., 2025): “For CMV, pre-emptive treatment of laboratory-detected viral reactivation with valganciclovir or ganciclovir should follow local or national guidelines, and treatment of CMV-related disease, which is exceedingly rare, is always recommended“. PCR-based monitoring for CMV is mandatory during the first 100 days (Sharrack et al., 2020).
-
“No cases of PML (Progressive Multifocal Leukoencephalopathy) have been reported after AHSCT for the treatment of MS” (Muraro et al., 2025).
Common Adverse Events Related to Infusion of Cryopreserved Stem Cells:
Cryoprotectants like dimethyl sulfoxide (DMSO) are essential for stem cell preservation, preventing ice crystal formation and cell death.
These AEs are linked to DMSO toxicity, dead cell debris, and electrolyte release from lysed cells. To mitigate risks, strategies such as premedication, proper hydration, controlled infusion speed, and, in some cases, washing the stem cell product—especially for vulnerable patients—can help reduce DMSO exposure. (Hematopoietic Stem Cell Transplantation for Neurologic Diseases. Chapter 9. Handbook of Clinical Neurology. Elsevier).
Following some studies, in which early adverse events have been reported in details:
MIST trial by Burt et al., 2015, evaluated 110 RRMS patients, comparing AHSCT vs. other DMTs with a follow-up for a median of 2 years.
There were no TRM and no early or late infectious cases (such as fungal, Pneumocystis jirovecii, CMV, Epstein-Barr virus, or JC virus). No patients who received AHSCT developed nonhematopoietic grade 4 toxicities (such as myocardial infarction, sepsis, or other disabling or potential life-threatening events).
Burman et al., 2014. Journal of Neurology, Neurosurgery & Psychiatry.
In this Swedish cohort of 48 pwMS underwent AHSCT: 34/48 had RRMS, and the mean follow-up time was 47 months. There was no mortality, while the most common long-term side effects were herpes zoster reactivation in 8 patients (17%): 4 during the first year; 3 during the second year; and 1 during the third year after AHSCT.
Nicholas et al., 2021. Neurology.
In the study by Nicholas et al., 2021, 120 patients were evaluated (52% PPMS or SPMS and 48% RRMS). As early complications “Almost 90% of the treated patients experienced at least 1 early complication after AHSCT”.
After mobilization, one cohort showed higher rates of fever, positive cultures, neutropenia, and readmissions, likely due to the higher cyclophosphamide dose (4 g/m² vs. 2 g/m²). During conditioning/HSCT, this cohort more frequently experienced fever, diarrhea, and EBV reactivation, while the second cohort had higher rates of severe nausea and vomiting.” CMV was detected in 26 out of 120 patients. EBV reactivation was demonstrated in 87 of 109 (80%; 11 missing/not tested) of participants after AHSCT.
Burt et al., 2022. Journal of Neurology.
The authors investigate the results of real-world application of non-myeloablative AHSCT in 507 patients at the Northwestern University (414 with RRMS and 93 with SPMS) between 2003 and 2019. The median follow-up was 5 years. Data on infection was divided into 3 different timeframes:
(A) During hospitalization: “the main infections were stool clostridium difficile (1.1%), one bacteremia (0.19%) without hypotension or sepsis speciated as Klebsiella pneumoniae that was sensitive to cefepime”. Burt et al., 2022
(B) Hospital discharge until day 100: “the most common infections involved mucosal surfaces infections from viral (n = 13) or bacterial (n = 18) URTI (upper respiratory tract infection), sinusitis (n = 12), or oral or vaginal candidiasis, and bacterial (n = 28) or viral (n = 3) UTI (urinary tract infection). All patients recovered without need for hospitalization. Transient viral hemorrhagic cystitis occurred in 3 patients: 2 from BK virus, and one from adenovirus. One patient developed clostridium difficile diarrhea”. Burt et al., 2022
(C) 100 days until one year post-AHSCT: “the most common infections were again URTI and UTI infections that resolved with oral antibiotics and occurred in 26 and 35 patients, respectively. Two patients developed clostridium difficile diarrhea. One patient developed a cutaneous breast implant gram positive bacterial infection. Dermatomal VZV infections occurred for the first time in 12 patients.” Burt et al., 2022
No patient at any time point (A, B or C) after AHSCT developed PML, CMV disease, Pneumocystis jiroveci pneumonia, or EBV symptoms or lymphoproliferative disease. No one has died from COVID 19 infection.
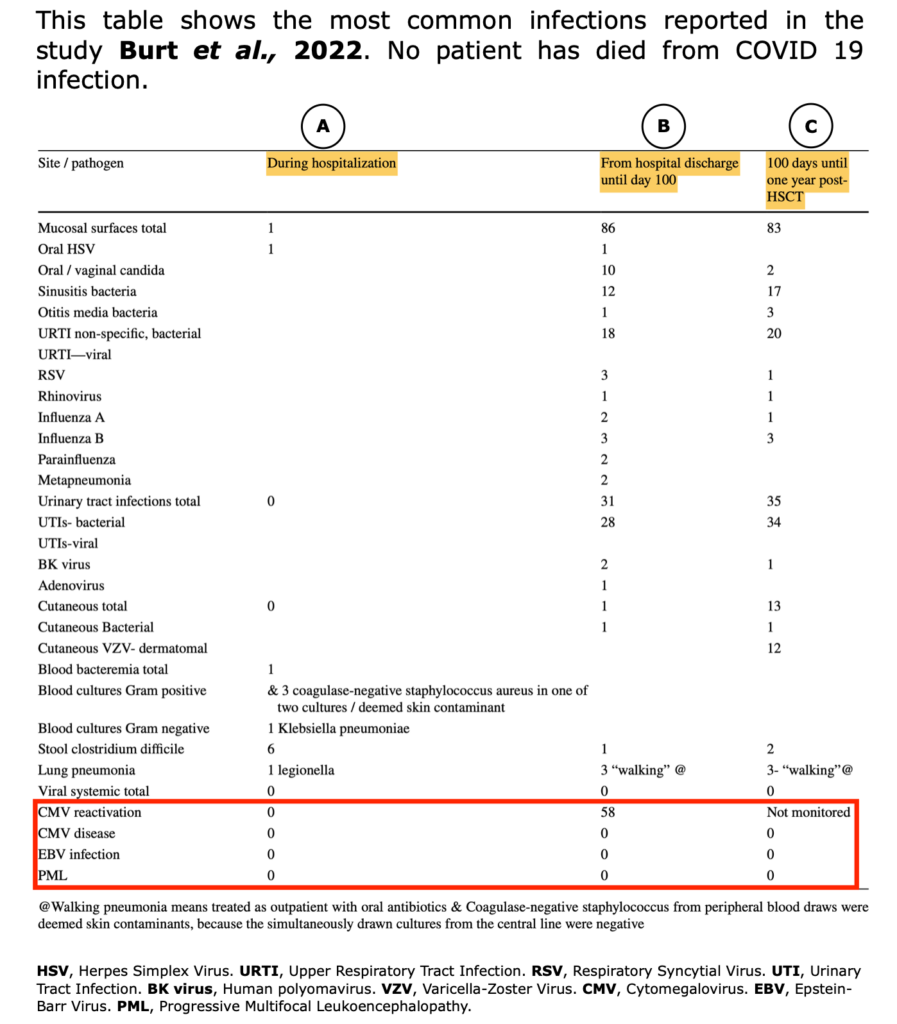
Table from Burt et al. “Real-world application of autologous hematopoietic stem cell transplantation in 507 patients with multiple sclerosis”. J of Neurol (2022)
Jespersen et al., 2023. Multiple Sclerosis and Related Disorders.
32 patients with RRMS were treated with AHSCT at the Danish MS Center (Rigshospitalet, Denmark) from May 2011 to May 2021. Seven patients underwent AHSCT with BEAM/ATG regimen with a median follow-up of 49 months, and twenty-five patients underwent AHSCT with the regimen of CY/ATG with a median follow-up of 39 months.
According to the authors “Reported adverse events during mobilization and conditioning were mainly mild to moderate and required no treatment.”
The most significant severe adverse events were anemia and neutropenic fever during conditioning, which were anticipated complications due to bone marrow suppression, consistent with similar studies using BEAM/ATG or CY/ATG.
No treatment-related mortality was reported in this study.
Transplant-Related Mortality
Within 100 Days After Conditioning Regimen
TRM are deaths within the first 100 days after a transplant. It is defined as death due to causes unrelated to the underlying disease (MS).
In this 20-year UK-wide study of 364 pwMS undergoing AHSCT, the TRM was 1.4% (5 patients: 2 PPMS and 3 RRMS) (Kazmi et al., 2025).
All TRM cases occurred within 100 days post-transplant and were associated with advanced baseline disability (4 out of 5 patients had an EDSS of 6.5, and 1 patient had an EDSS of 6.0). Causes of death included cardiac arrest, sepsis, and respiratory failure, primarily during or shortly after the conditioning phase. These findings underscore the importance of careful patient selection and pre-transplant evaluation to minimize risks.
As the authors note “This report, for the first time, confirms no benefit and potential risks of higher ATG doses (>6.0 mg/kg). Therefore, it seems reasonable to cap the rATG dose to 6.0 mg/kg.”.
This aligns with data showing increased complications at higher rATG doses, supporting the recommendation to limit the dose to improve safety and reduce toxicity.
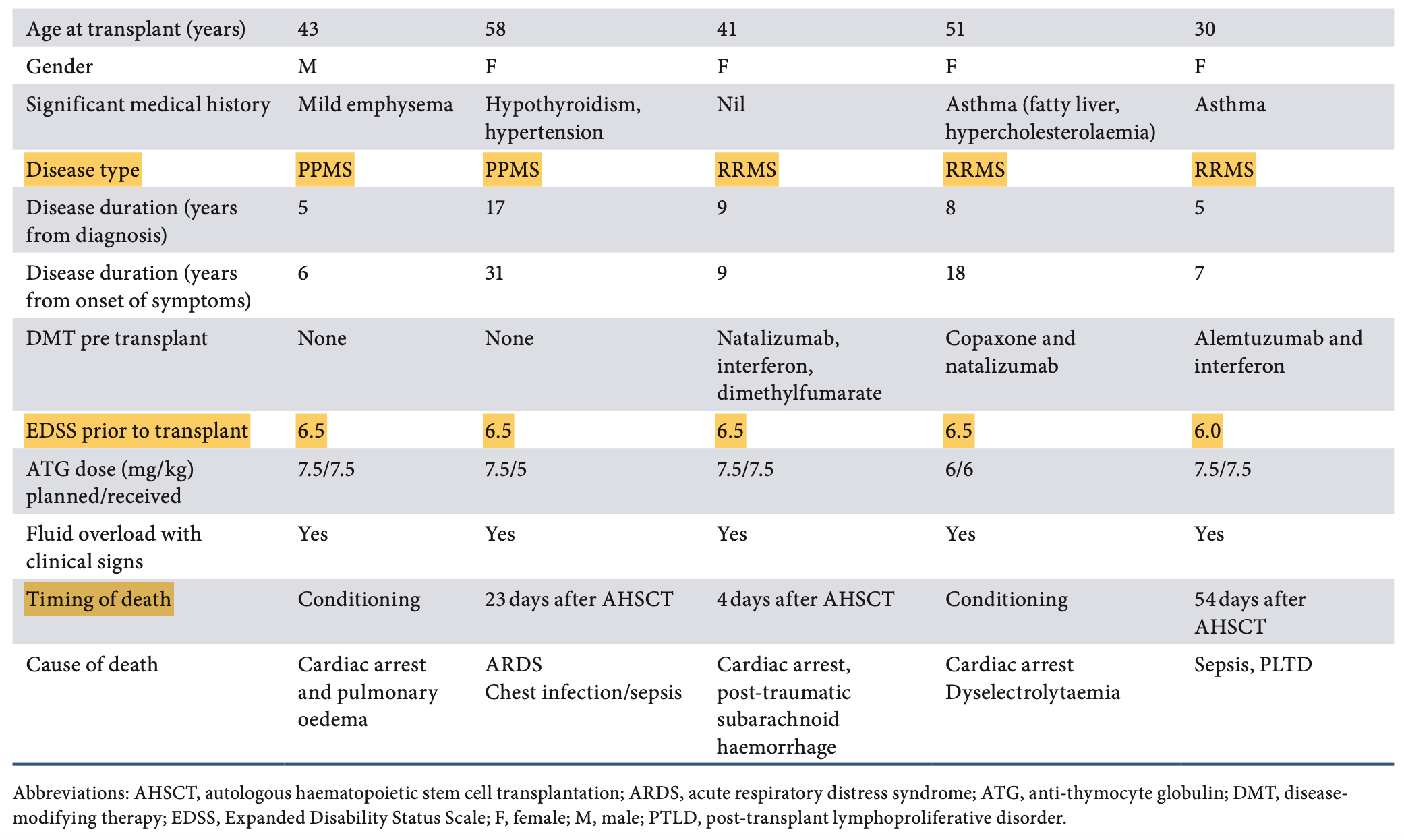
Table from Kazmi et al., 2025: TRM occurred in 5 out of 364 patients—2 with PPMS and 3 with RRMS.

Source: EBMT handbook 2024
An analysis of the EBMT registry indicated that TRM rates significantly decreased over time: from 7.3% during 1995-2000, to 1.3% between 2001-2007, and falling to less than 1.0% in the period from 2008 to 2016 (Muraro et al., 2017).
In 2022, an update of the EBMT registry (Alexander et al., 2022) emphasized that “reduced intensity conditioning regimen significantly reduce the risk of treatment-related morbidity such as infections, infertility, organ damage, as well as treatment-related mortality (TRM) to 0.2%. Indeed, there was chronological improvement in HSCT outcomes (i.e., progression-free survival, relapse/progression, and TRM), strictly connected to the transplant center experience, patient selection and progress with supportive care”.
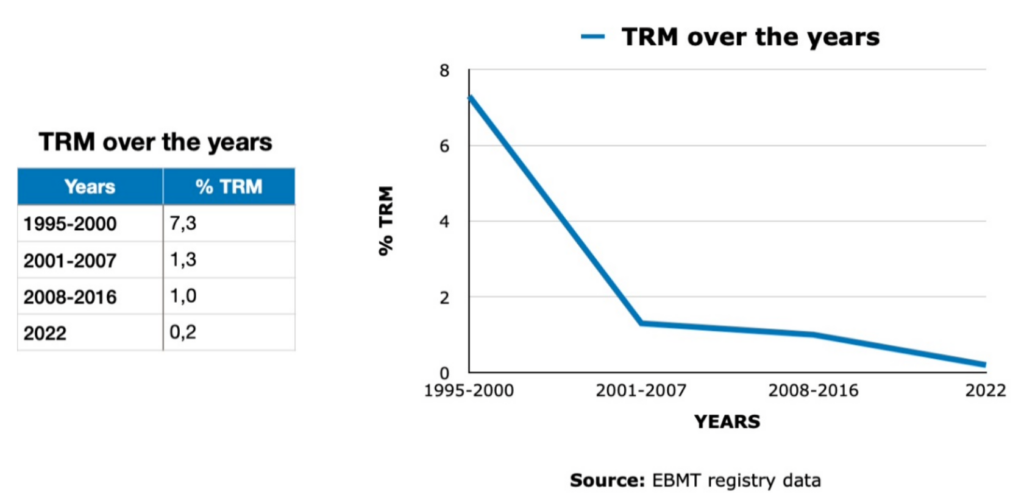
Figure created by curems.net based on the EBMT registry
Unfortunately, there were 5 late non-AHSCT-related deaths:
- 3 died more than one year after AHSCT from a cerebrovascular accident related to medication non-compliance (1 patient), a myocardial infarction (1 patient), and (1 patient) during an elective cholecystectomy (unknown cause);
- 1 patient died 3 years after HSCT from colon cancer;
- 1 patient who received alemtuzumab in the conditioning regimen died 10 years after AHSCT from a T cell lymphoma.
No patient developed post-AHSCT diseases such as myelodysplastic syndrome, leukemia, or bladder cancer.
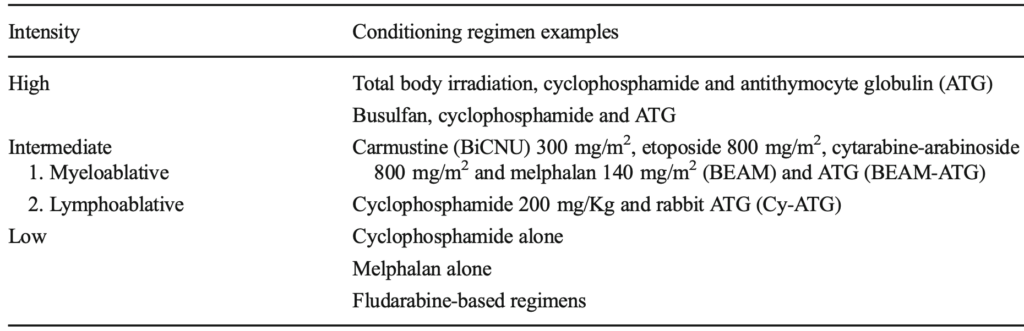
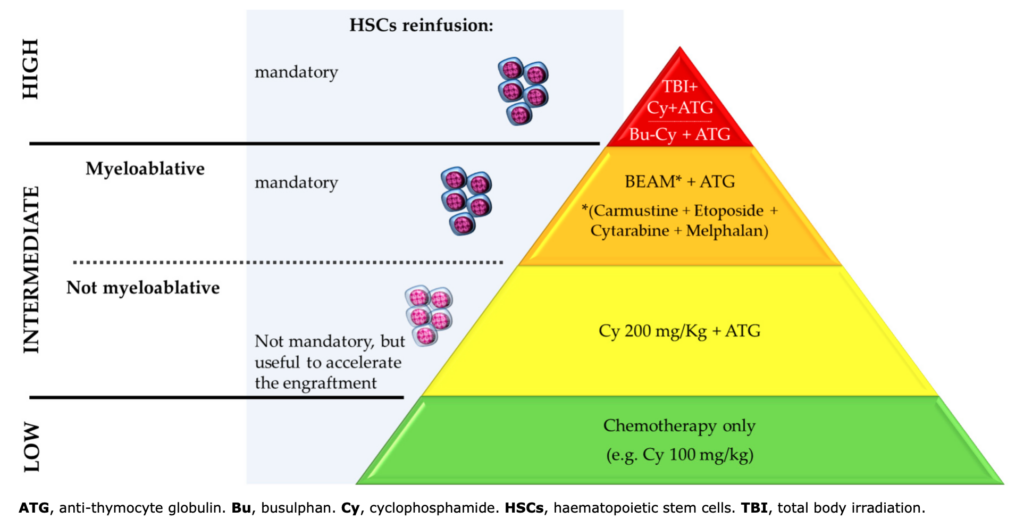
Willison et al. published an extended overview of clinical trials treating pwMS with AHSCT. On the section dedicated to risks, they reported that:
“The percentage of total patients who underwent transplantation [AHSCT] and died as a consequence, with deaths related to conditioning regimen, was 2.4% following a high-intensity regimen (2 deaths, 85 patients), 1% following myeloablative intermediate-intensity conditioning (5 deaths, 491 patients), 0.1% following lymphoablative intermediate-intensity conditioning (1 death, 1065 patients) and 0% following low-intensity conditioning (0 deaths, 42 patients)”.
See the table below for a summary.
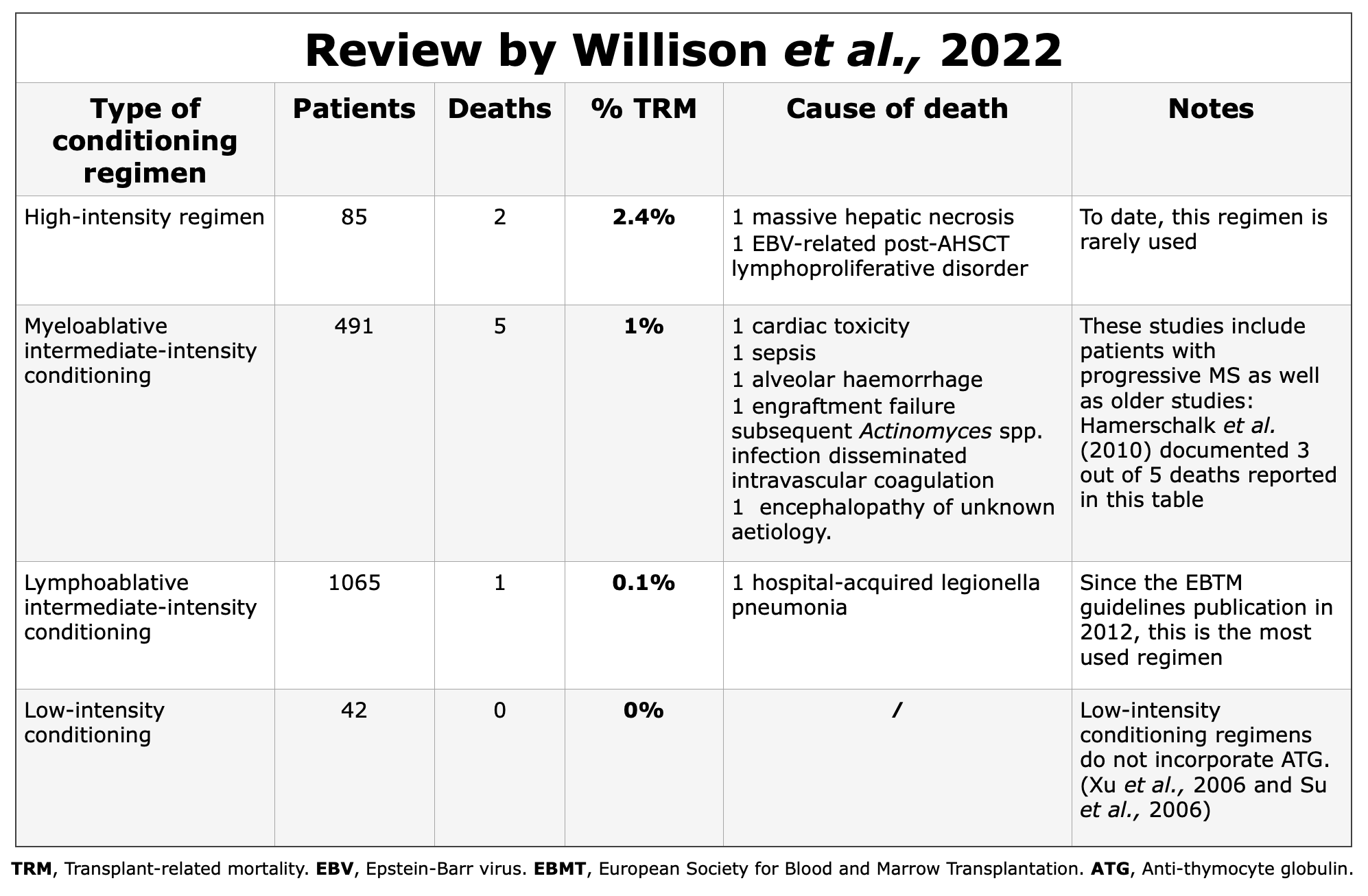 Figure created by curems.net based on data reported by Willison et al., 2022
Figure created by curems.net based on data reported by Willison et al., 2022
Late Adverse Events
“Late effects following AHSCT may result from the transplant regimen and altered post-transplant immune reconstitution, but may also be driven by pre-treatment of the underlying neurological disease.” (Muraro et al., 2017) (Sharrack et al., 2020).
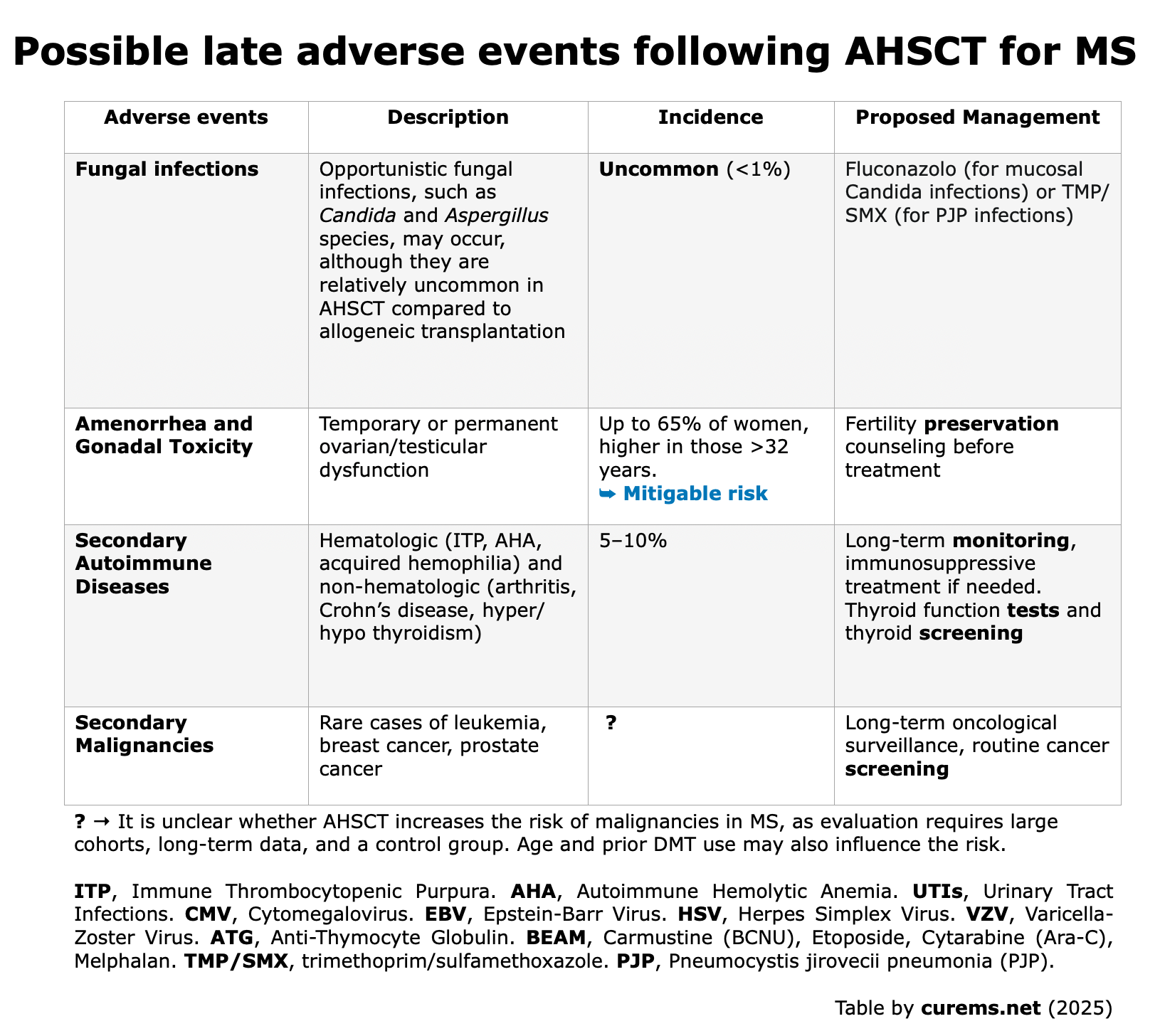
The most common late adverse events post-AHSCT are:
- Fungal infection
- Loss of fertility and amenorrhea
- Autoimmune diseases
- Secondary malignancies
Data obtained from “Hematopoietic Stem Cell Transplantation for Neurologic Diseases“. Chapters 8-10. Handbook of Clinical Neurology (Elsevier, 2024). Edited by Professors M. Inglese and G.L. Mancardi

Fungal Infections
Fungal infection are uncommon (<1%) after AHSCT. According to Mikulska et al. (Hematopoietic Stem Cell Transplantation for Neurologic Diseases. Chapter 10. Handbook of Clinical Neurology. Elsevier), there’s a specific need to prevent PJP (Pneumocystis jirovecii pneumonia) due to its higher risk in immunocompromised patients. Other fungal infections, like oral (thrush) or esophageal Candida, are more frequent but less severe, while serious mold infections (e.g., invasive aspergillosis) are rare.
Fertility & Amenorrhea
In women of child-bearing age, AHSCT can negatively impact reproductive health since the ovaries are especially vulnerable to alkylating agents like cyclophosphamide or melphalan, which are frequently used in the conditioning regimens for MS (Snarski et al., 2015) (Das et al., 2019).
Fertility counseling is highly recommended: we emphasize that before initiating transplant, it is essential to consider and discuss the potential impacts on the patient’s future fertility.
This strategy should include an exploration of fertility-preserving strategies for both females or males and a dedicated consultation with a physician specialized in reproductive medicine (Salooja et al., 2024 – EBMT handbook).
In females post-AHSCT, the incidence of persistent amenorrhea varied from 30% in a group of 43 women treated with mixed conditioning regimens (BEAM-ATG or Cy-ATG) in Massarotti et al., 2021, to 43% in a group of 30 patients who underwent the Cy-ATG protocol (Kvistad et al., 2019).
Regarding the menstrual cycle resumption, in the study by Massarotti et al., 2021, 30 out of 43 patients, recovered menses after a mean time of 6.8 months; no differences were detected among different conditioning regimens’ intensity (BEAM-ATG or Cy-ATG), although the sample size was small (43 women).
In this study, older age at the moment of AHSCT and previous pulsed use of Cy were identified as predictors of persistent amenorrhea in the study.
Burman et al. (2014) during the follow-up period (with a mean follow-up time of 47 months), there were a total of 8 pregnancies among 4 women (from a cohort of 26 wMS included in this study). Of these pregnancies: 5 resulted in healthy infants (including one set of twins). There were also 2 spontaneous abortions and 1 ectopic pregnancy. Additionally, one legal abortion was performed. Moreover, 1 man fathered a healthy child through IVF with cryopreserved semen, and 1 woman gave birth to a healthy infant following IVF with cryopreserved eggs after an otherwise normal pregnancy.
In the study by Zafeiri et al. (38 patients aged 20-44 years), 7 patients out of 38 female patients became pregnant post-AHSCT: 6 spontaneously, 1 both spontaneously and with IVF. The study measured AMH levels as a “biomarker of fertility” reflecting the ovarian reserve in females.
Anti-Müllerian Hormone: A brief insight
Anti-Müllerian Hormone (AMH) is linked to the presence of growing follicles during the menstrual cycle. Recently, AMH has been increasingly utilized as a biomarker of fertility.
It is considered superior to FSH and E2 in assessing ovarian reserve due to its relative stability throughout the menstrual cycle. Initially, it was believed that AMH levels were unaffected by contraceptive methods or anovulation. However, various studies have questioned its stability. Consequently, the use of AMH as a fertility biomarker should be contextualized within the patient’s overall medical history. (Cedars MI, 2022)
This the main reason why AMH is an excellent predictor of quantity and not quality, and thus does not predict pregnancy success (Granger et al., 2019).
Nevertheless, age still continues to be the best indicator of pregnancy success (i.e., the chance to conceive decreases with age in both females and males).
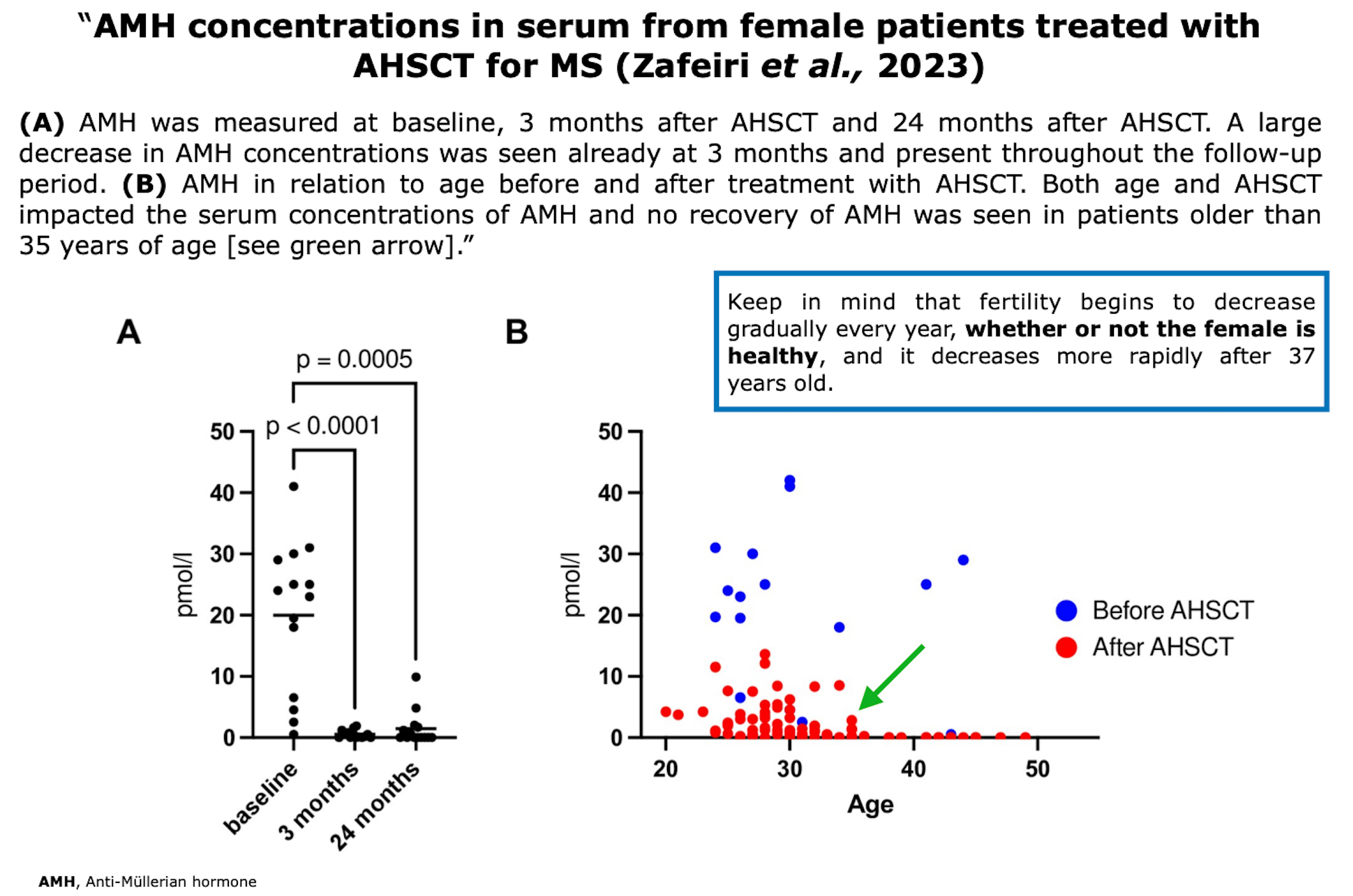
Figure from Zafeiri et al. ”Anti-Müllerian hormone and pregnancy after autologous hematopoietic stem cell transplantation for multiple sclerosis”. PLoS ONE (2023)
Fertility preservation in males
Limited data are available on male infertility (Tichelli et al., 2014). AHSCT could represent a risk, depending on patient characteristics and the conditioning regimen used.
“Sperm cryopreservation is an established fertility preservation option for post-pubertal boys and men. Sperm can be used either for artificial insemination or, if the quantity and/or quality of sperm are insufficient, for intracytoplasmic sperm injections for in vitro fertilization.” (Salooja et al., 2024 – EBMT handbook).
In the study Mariottini et al. (2021) 29 patients (6 males and 23 females) were monitored before undergoing AHSCT (27 with BEAM/ATG and 2 females received a reduced regimen). 17 out of 29 had received chemotherapy-based immunosuppression.
All 6 male patients received BEAM+ATG regimen. “In males post-AHSCT testosterone levels were within normal range in 5 out 6 available cases. Testosterone levels at follow-up were not reduced compared to baseline in 2/3 (67%) cases who had the baseline assessment.”
Fertility preservation in females
AHSCT can deeply impact fertility. According to Salooja et al., 2024 – EBMT handbook, the most common techniques for fertility preservation in females before undergoing AHSCT are:
- Embryo and Oocyte Cryopreservation: Carbone et al., 2023
- Gonadotropin-Releasing Hormone Agonists (GnRHa): Several reports focus on the increasing risk of relapses with GnRHa; however, a recent review that included 225 women undergoing a total of 338 IVF procedures showed that there are no risks of relapses if DMTs are maintained until IVF (Mainguy et al., 2022).
- Ovarian Tissue Cryopreservation (OTC): Colmorn et al., 2023
Here an extended review on fertility preservation from an expert panel: “Assisted Reproductive Techniques in Multiple Sclerosis: Recommendations from an Expert Panel” (Oreja-Guevara et al., 2023).
Secondary AIDs
According to Johns Hopkins Medicine “Autoimmune disease [AIDs] happens when the body’s natural defense system can’t tell the difference between your own cells and foreign cells, causing the body to mistakenly attack normal cells. There are more than 80 types of autoimmune diseases that affect a wide range of body parts”. Autoimmune diseases have a high prevalence: here is a lay version about the incidence of AIDs worldwide from Scientific American (2021).
Secondary autoimmune diseases (AIDs), it is meant the risk of developing another AIDs as a consequence of the AHSCT (i.e. where the first AIDs is MS). Modifications resulting from the induced immunologic resetting after AHSCT, alongside a persistent genetic background, may potentially trigger secondary AIDs.
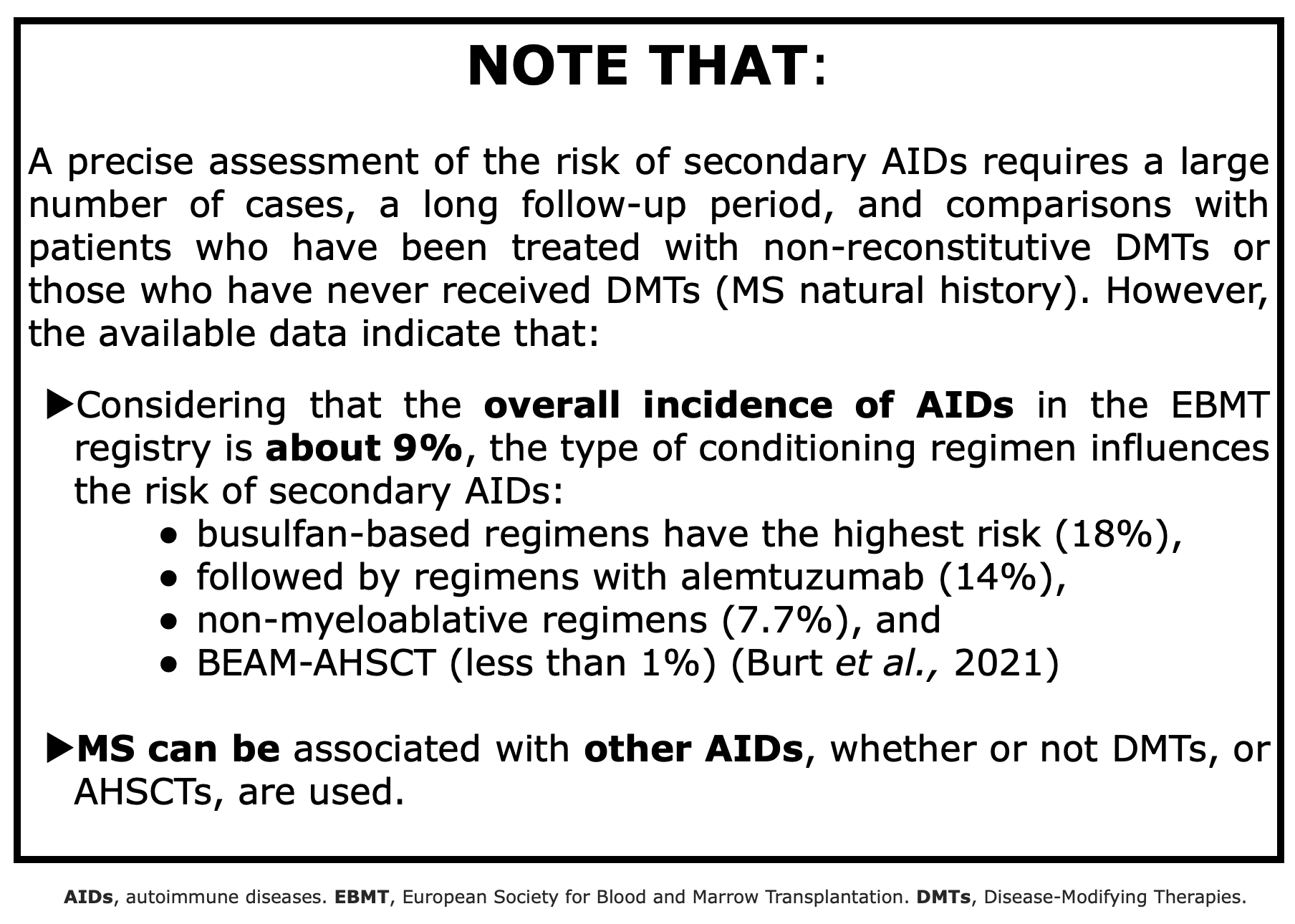
Table created using data from Burt et al., 2021
As stated by Currò et al. (2016) “several mechanisms have been proposed to justify the occurrence of these adverse events, such as:
- the loss of peripheral tolerance after conditioning regimen,
- the proliferation of autoreactive cells by homeostatic expansion, and
- the failure of negative selection during de novo thymic ontogenesis of T lymphocytes.”
Secondary Malignancies
There is a potential increased risk of developing cancers due to the high-dose chemotherapy used in the conditioning regimen. At the moment it is not known if AHSCT in MS is associated with increased long-term risks cancer, because the evaluation of the risks needs very large number of patients, long-term data and a control group (Muraro et al., 2025).
Read here for the Global cancer facts & figures 5th by the American Cancer Society: It is important to keep in mind that in the general population “approximately 1 in 5 individuals will develop cancer in their lifetime, and 1 in 9 men and 1 in 12 women will die from the disease [cancer]”
Additionally, it should be noted that the risk of cancer may be influenced by the patient’s age and the DMTs taken prior to transplant. “However, since most autoimmune disease patients have already been heavily treated with several immunosuppressive regimens, and since the autoimmune disease itself may predispose to development of malignancies, it is difficult to define the exact influence of AHSCT in this scenario” (Arruda et al., 2017).
Other Key Considerations
- Hospitalization and Recovery: The procedure requires a lengthy hospital stay and a prolonged period of recovery.
- Psychological Impact: The stress and psychological burden associated with such an intense treatment can be significant in some patients.
- The selection of patients is very important: AHSCT failure and a continuous worsening of disability can have a significant psychological impact. Therefore, patients must be carefully selected and psychologically prepared.
Read here “AHSCT: Patients’ Stories” for more details on this topic.