AHSCT as an MS cure
The AHSCT holds the potential to being a “cure” for MS
✅ Related links: “Working definition of cure MS“.
Rationale of AHSCT
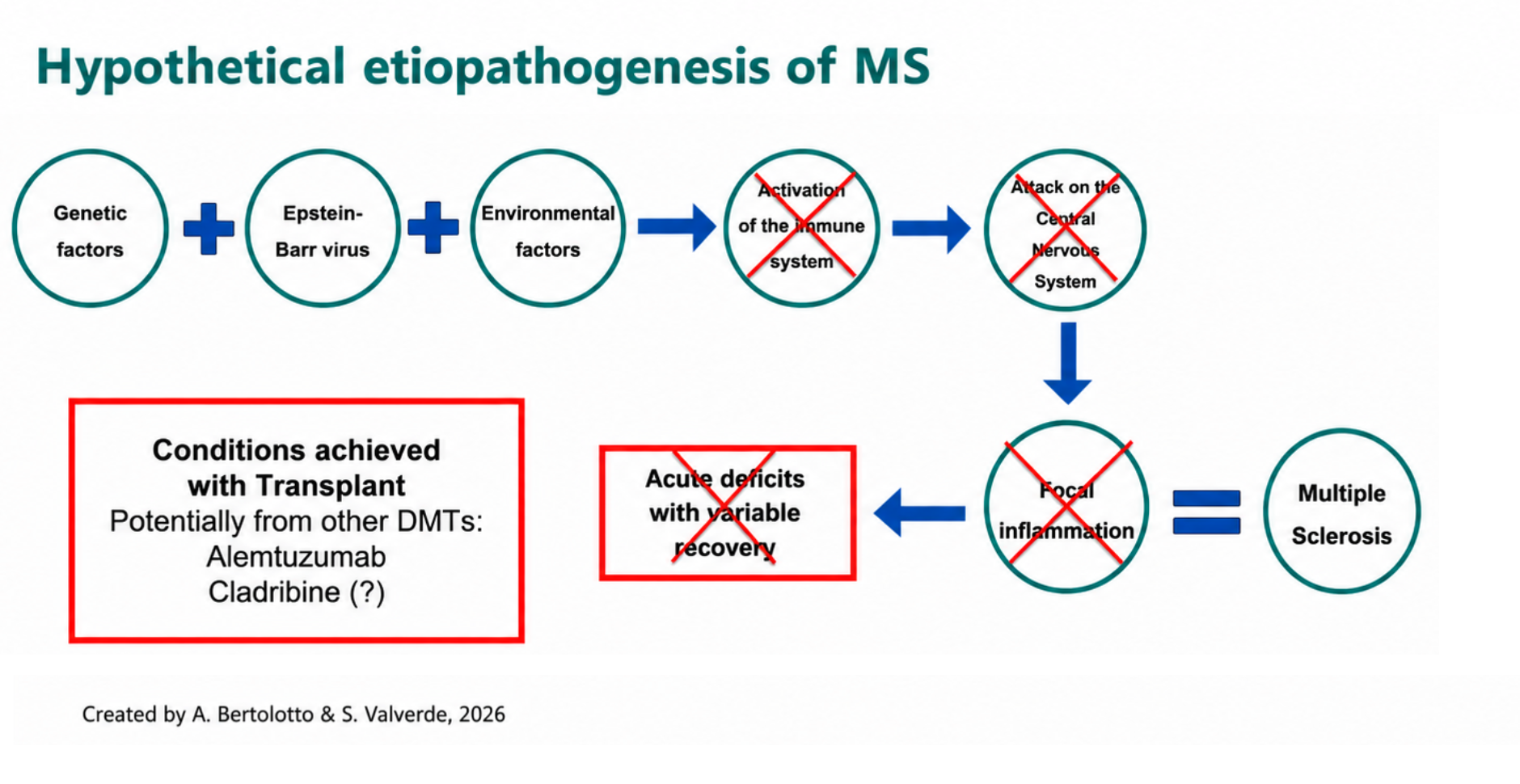
MS develops through a combination of genetic predisposition, EBV (Epstein-Barr Virus) infection, and environmental factors (childhood obesity, vitamin D deficiency, smoking, pollution, gut microbiota alterations, among others not yet fully defined). Together, these conditions drive the immune system — normally responsible for defending the body against pathogens — to become aggressive toward the patient’s own CNS. This occurs through the production of autoantibodies and, subsequently, auto-aggressive lymphocyte clones capable of attacking the myelin. When these clones multiply and enter the CNS, they cause inflammation, leading to new lesions on MRI and, in many cases, clinical relapses.
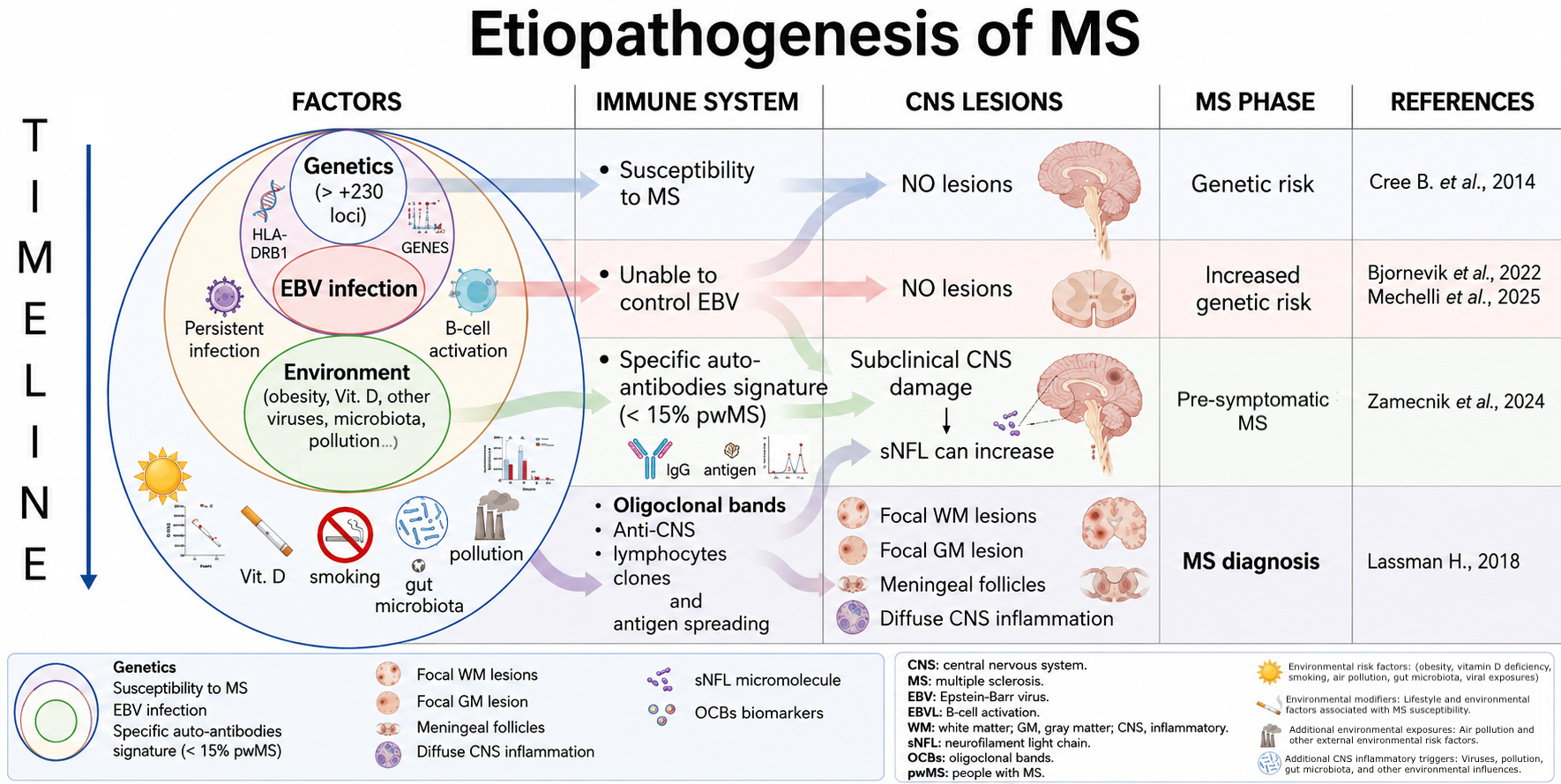
AHSCT (Autologous Hematopoietic Stem Cell Transplantation) is designed to interrupt this mechanism at its root: by eliminating the auto-aggressive immune cells responsible for CNS damage and reconstituting the immune system from the patient’s own hematopoietic stem cells, AHSCT aims to produce a new, “re-educated” immune system that no longer recognizes the CNS as a target.
Other therapies, such as Alemtuzumab (Lemtrada) and Cladribine (Mavenclad), are also classified as IRTs (Immune Reconstitution Therapies) and share this general principle of immune reset. However, the strongest scientific evidence supporting the possibility of achieving an MS “cure” comes specifically from AHSCT studies — which is why this website focuses on this procedure.

Mancardi et al., 2018
What is AHSCT?
AHSCT is a one-time procedure for appropriately selected patients, involving sequential steps from pre-transplant assessment through immune reconstitution.
Procedure overview
- Patient selection — Eligibility is assessed against established clinical criteria (see eligible patient section).
- Informed consent — The procedure, risks, and alternatives are discussed in full before consent is signed.
- Pre-transplant workup — Haematological, immunological, infectious, cardiological, and neurological assessments are completed to minimise risk. Fertility preservation is offered to eligible patients of both sexes.
- Mobilisation — Cyclophosphamide and G-CSF are administered to mobilise haematopoietic stem cells (HSCs) from the bone marrow into the bloodstream, while concurrently reducing autoreactive immune cells.
- Leukapheresis — HSCs are collected via leukapheresis, a procedure analogous to blood donation in which a machine separates HSCs from other blood components.
- Cryopreservation — A minimum of 3 × 10⁶ CD34+ cells/kg body weight is required for reinfusion; collected cells are frozen until needed.
- Conditioning — An immunoablative regimen — classified per EBMT guidelines as high-, intermediate-, or low-intensity depending on myeloablative potential — is administered to eliminate autoreactive lymphocyte clones, including those targeting the CNS. Conditioning requires inpatient hospitalisation of approximately 1.5–3 weeks in a haematology unit. See conditioning regimens for details.
- Reinfusion — The patient’s own HSCs are reinfused intravenously. They migrate to the bone marrow and begin regenerating new blood and immune cells with reduced CNS reactivity. New white blood cells typically appear within 7–14 days; full immune reconstitution develops over subsequent weeks and months.
- Post-transplant management — Prophylactic antibiotics, antifungals, and antivirals are administered to prevent infection during the period of immune suppression; vaccination schedules are subsequently restored.
✅ For a shorter version of the video, click here.
Patient’s Right to Be Informed
Patient’s Right
to Be Informed
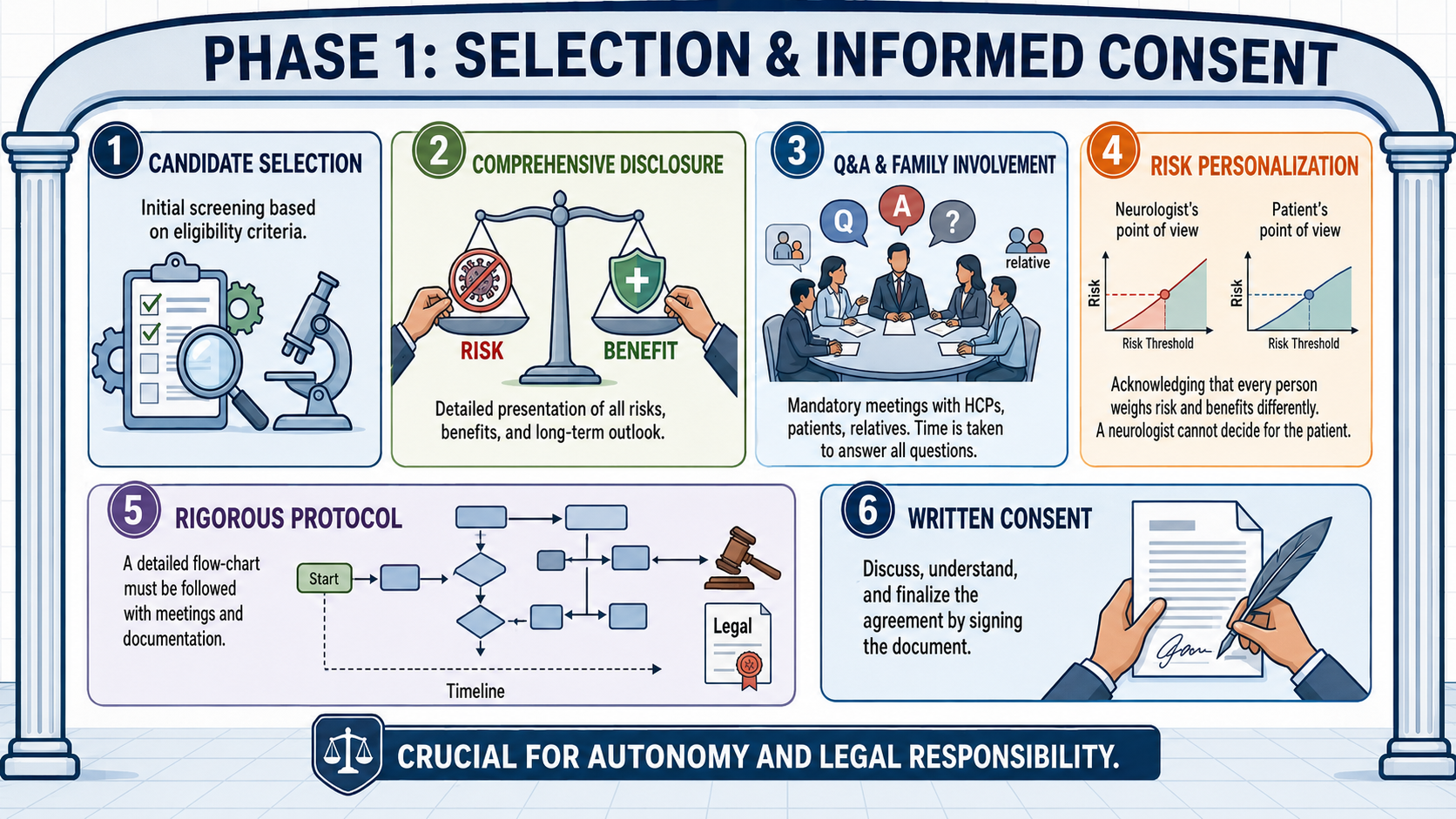
The following is Dr. Bertolotto’s personal opinion, based on his experience:
- Neurologist MUST explain and illustrate at the pwMS all the treatment options, including AHSCT.
- The evaluation and the weight of the risk is personal, everyone weights risk and benefits in a different way. Also the neurologist weight risk and benefit of the pwMS they have in front, but from his personal point of view; his personal evaluation can not replace that of the patient.
- Neurologist do not have the right to take a decision instead of the patient, in particular for treatment with risk of death; neurologists can not choose “a priori” the patient who will be offered AHSCT or DMTs. If a patient ask me “doctor, what would you do if you were in my shoes?” I explain my choice, but I add, “if you ask another neurologist it is very likely that you will receive a different answer, as the evaluation of risks and benefits is very personal”.
- Legal problems and responsibility: before AHSCT a detailed flow-chart must be followed, with meetings among HCPs and patient (and relatives), written informed consent, answers to all the questions. This procedure takes time, a lot of time, but it is time-saving considering that the management of post-AHSCT is, in the great majority of cases, very easy for many years.
- To present AHSCT to pwMS is not only a respectful approach, but also prevents the future accusation of wrong information to pwMS.
- We need an up-date of the 2013 working definition of “cure of MS” (Banwell et al., 2013).
- Progression of disability: the pwMS must be informed, from the time of communication of the diagnosis, that he/she has a RISK of progression.
✅ Articles Worth Reading: here an insightful article by Prof. Giovannoni (AHSCT vs. Alemtuzumab).
AHSCT Eligible Patient
The name of this website may suggest that AHSCT offers a path to “cure” for all people with MS. An important clarification is needed: AHSCT cannot repair established CNS damage, carries greater risk with older age and higher disability, and is not indicated for progressive MS without evidence of active inflammation (relapses or new MRI lesions).
As the 2023 German expert consensus states: “For advanced disease stages with a long duration, older age and greater impairment, data argue against a benefit that would justify the risks of transplantation” (Bayas et al., 2023).
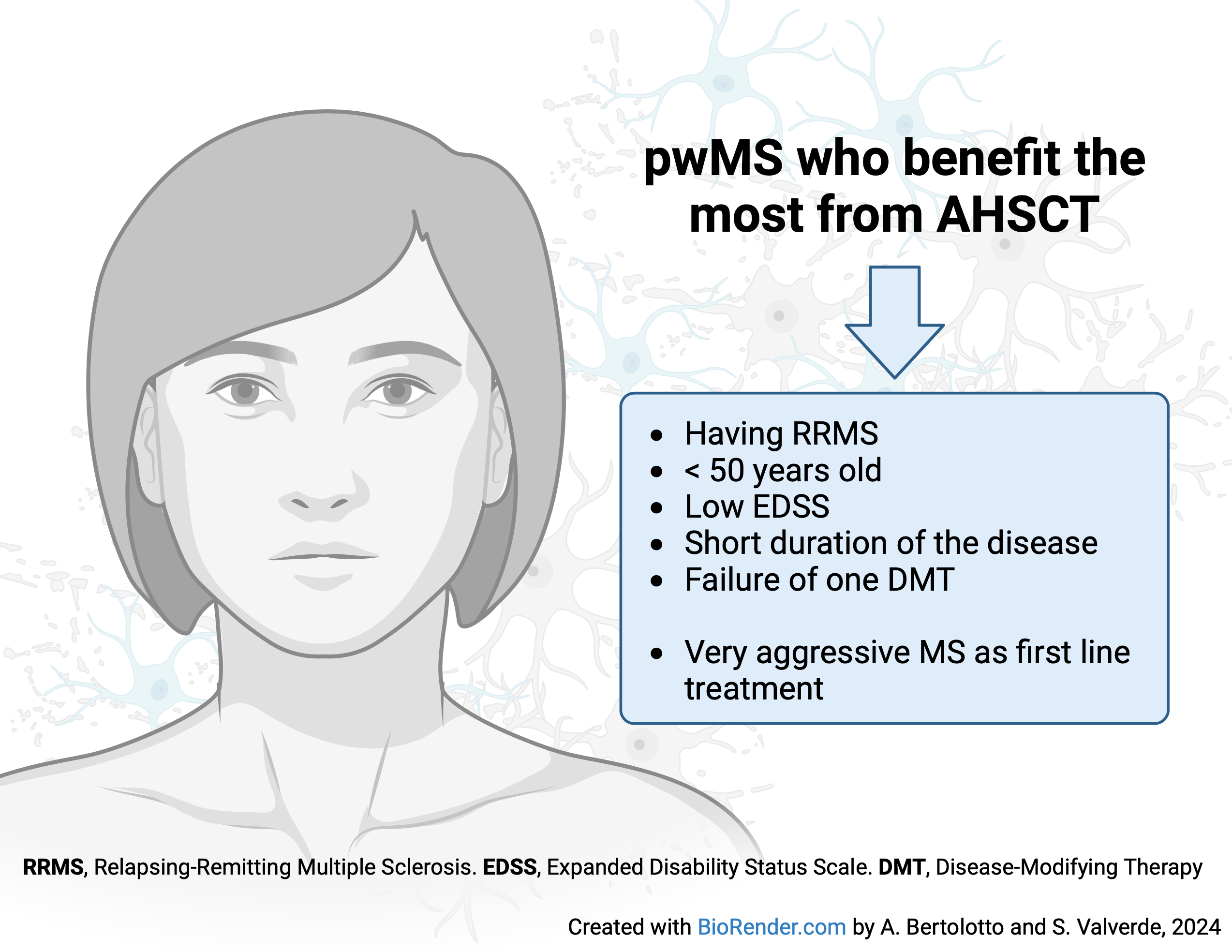
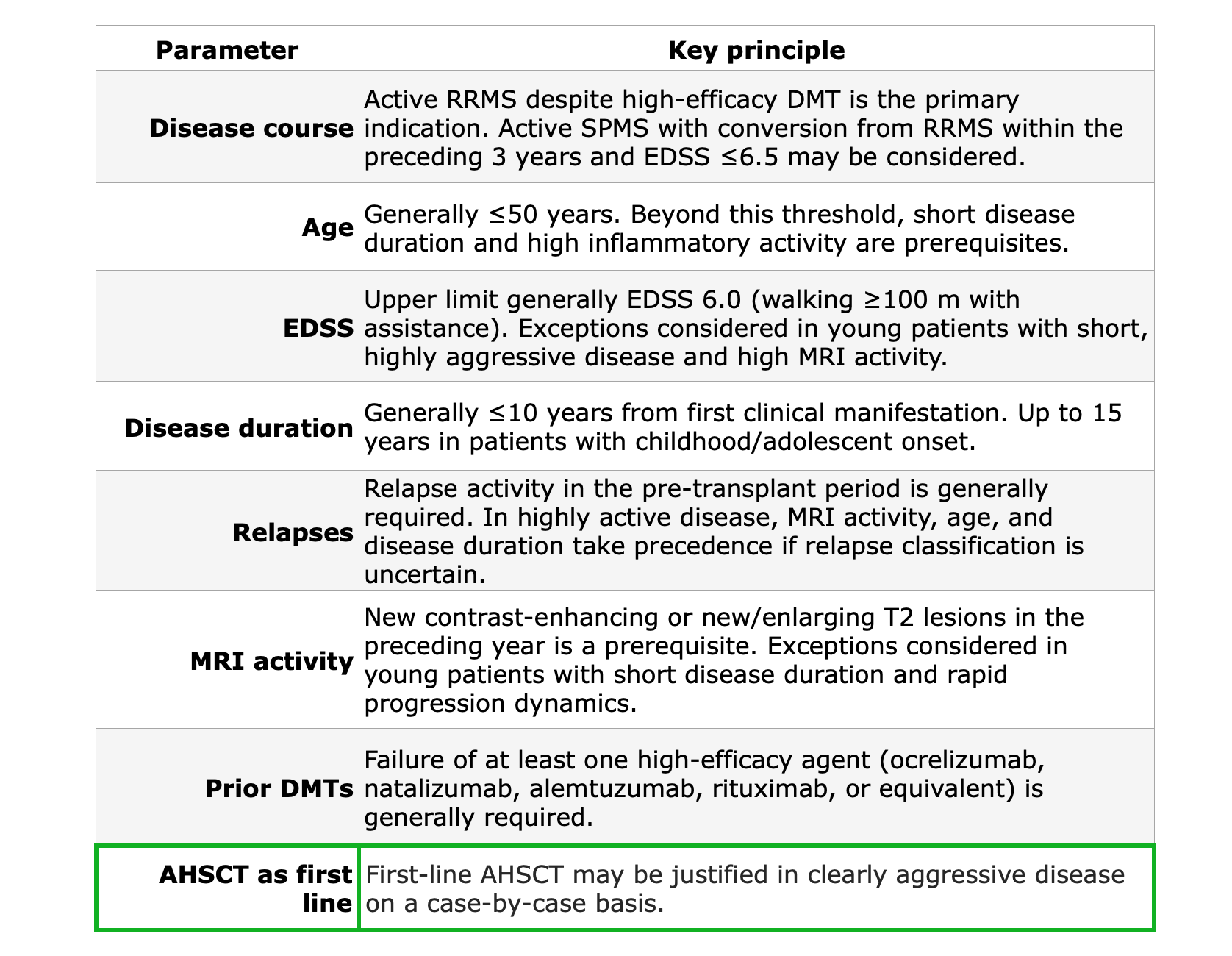
Eligibility criteria are evolving. AHSCT was initially reserved for patients who had failed all available DMTs. It was later extended to RRMS after failure of at least two DMTs. Currently, some trials enrol patients after a single DMT failure, and case reports support its use as first-line treatment in highly aggressive MS (Das et al., 2021). The most recent ECTRIMS/EBMT recommendations are provided in Muraro et al., 2025.
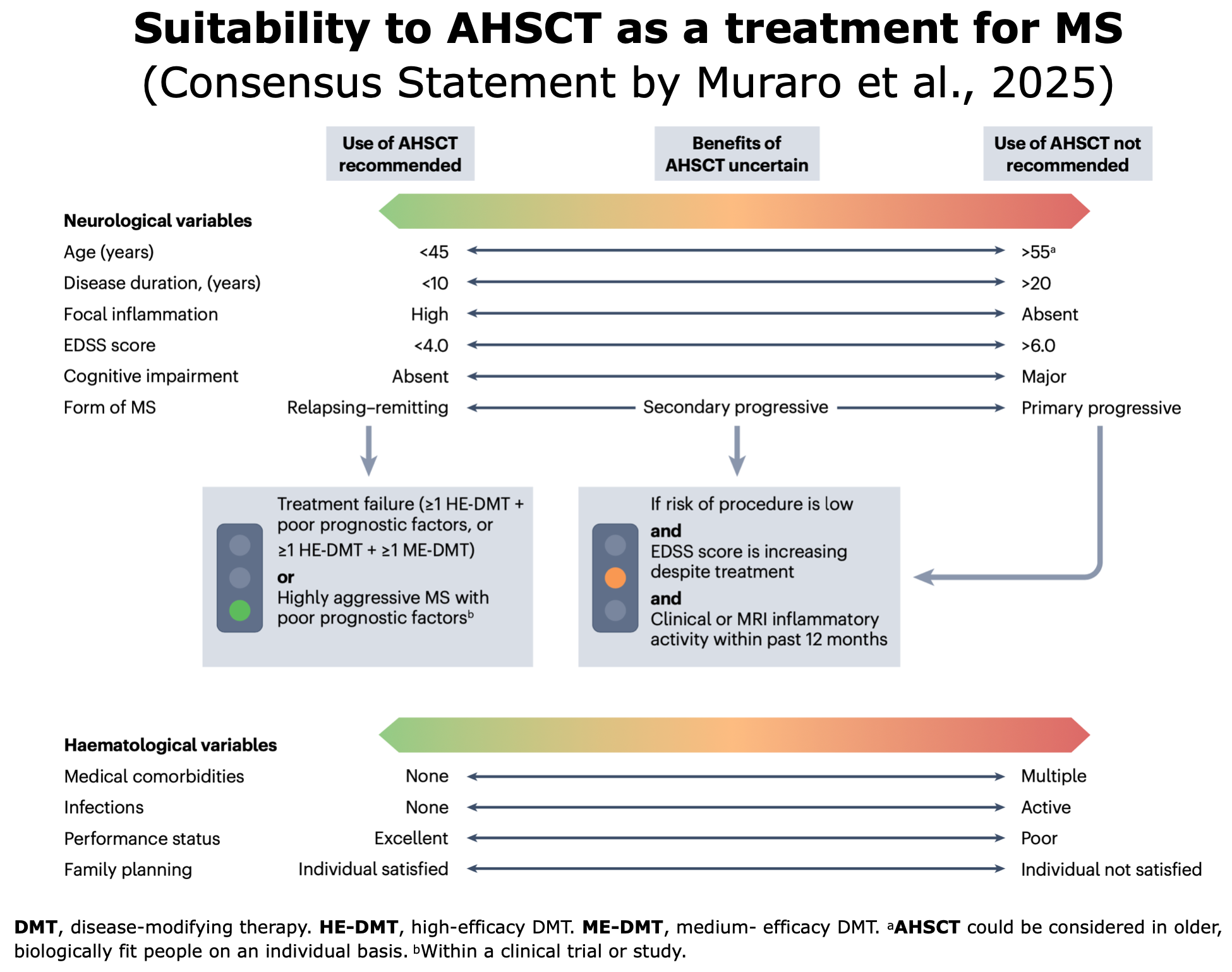
Figure from Muraro et al. “Autologous haematopoietic stem cell transplantation for treatment of multiple sclerosis and neuromyelitis optica spectrum disorder — recommendations from ECTRIMS and the EBMT“. Nature Rev Neural (2025).
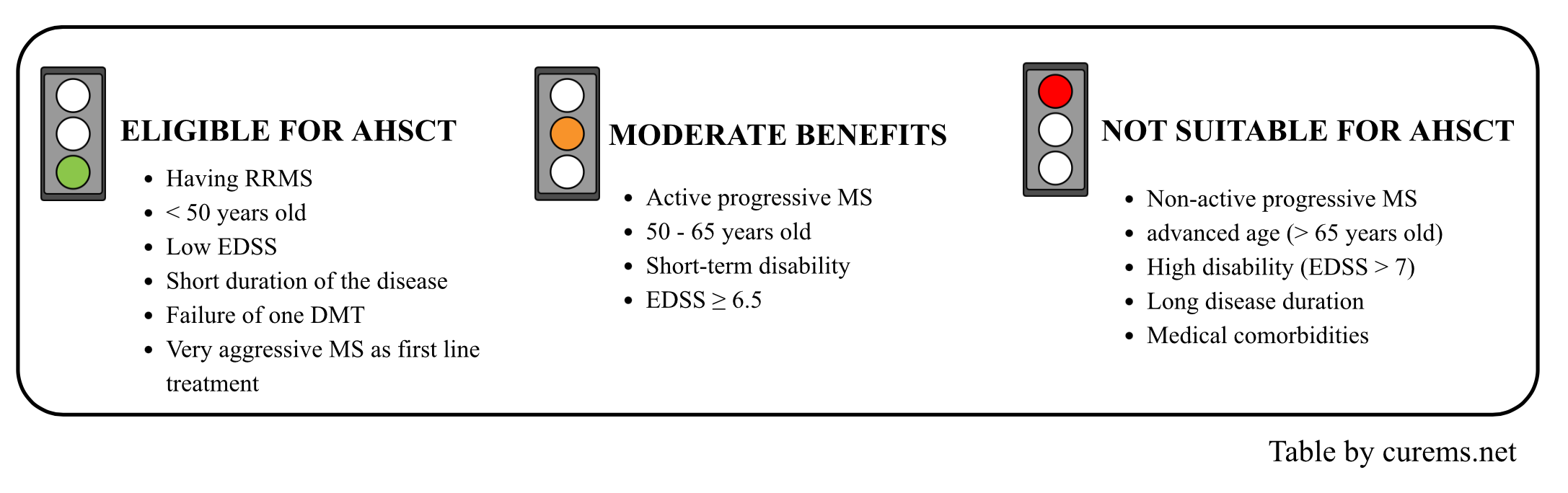
The numbers—age, disease duration, and Expanded Disability Status Scale (EDSS) score—are provided as illustrative examples to convey the principles and should not be considered strict cut-off values. Consequently, the profile on the far left (in green) represents the optimal candidate for AHSCT.
✅ Useful links: AHSCT in numbers
Clinical and Radiological Criteria for AHSCT Eligibility
Before undergoing AHSCT, several points need to be taken into consideration. We present an evaluation of various parameters used by a group of German experts.
The German expert group (Bayas et al., 2023) defines two tiers: core criteria (essential eligibility requirements) and extended criteria (additional factors that may broaden or refine the indication on a case-by-case basis). For main parameters see table.
Several parameters must be taken into consideration, in particular
- The clinical characteristic of the pwMS: the disease course of MS, age, EDSS, duration of illness, clinical and MRI activity in the last years, speed of clinical progression, therapy failure. (Bayas et al., 2023).
- The risk of adverse effects: TRM, the risk to fertility, infections, appearance of new auto-immune diseases, the long-term risks of cancer. Read here more about risks.
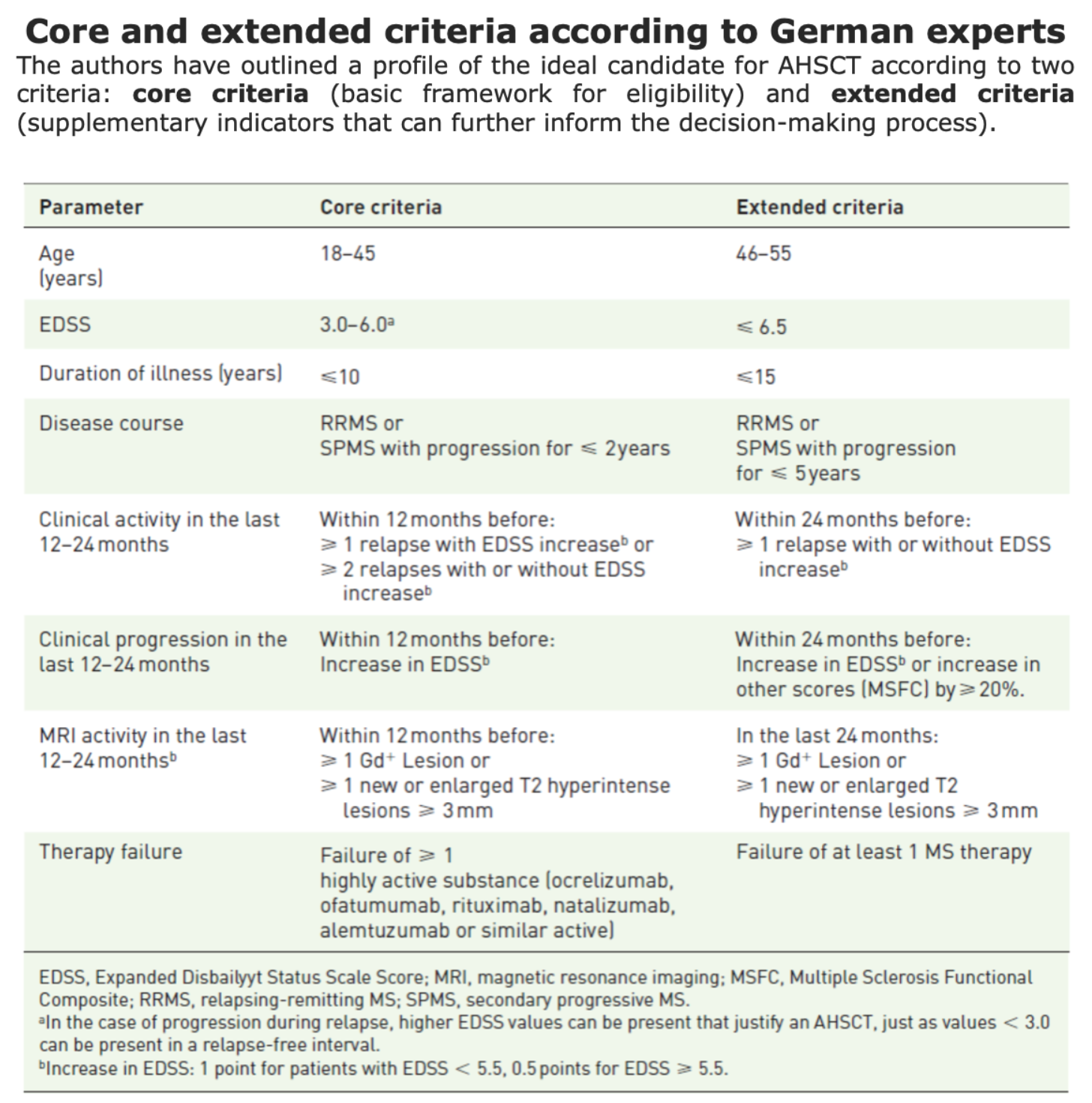
Table from Bayas et al. “Autologous haematopoietic stem cell transplantation for multiple sclerosis: a position paper and registry outline“. Therapeutic Advances in Neurological Disorders (2023)
Clinical criteria for AHSCT (Bayas et al., 2023)

Types of MS and AHSCT
The course of MS is classically subdivided in 3 forms: RRMS, SPMS and PPMS.
The great majority of these subsets do not have a single accepted definition and some of them are overlapping. For example, it is hard to distinguish among “Malignant” “Aggressive” and “Highly Active” MS. To reduce the confusion, each scientific paper specifies its particular definition.
An attempt to define the aggressive forms of MS is presented by Boffa et al., 2025: see figure below.
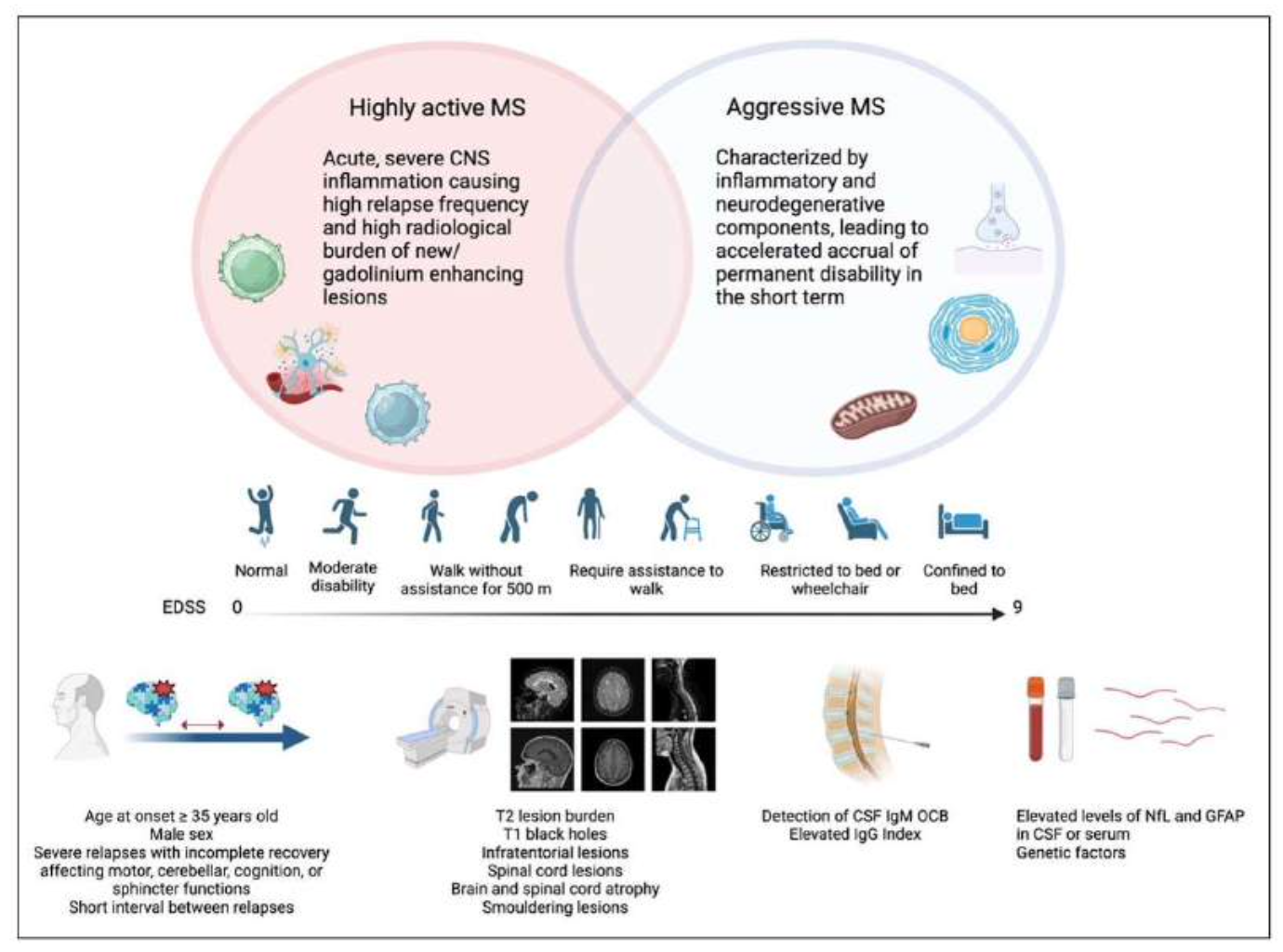
Differences between ‘highly active MS’, characterized by severe CNS inflammation responsible for heightened disease severity in the short term, and ‘aggressive MS”, encompasses both inflammatory and neurodegenerative components. Clinical, radiological and biological markers predicting the risk of highly active and aggressive MS. Figure by Boffa et al., 2025
Currently, the classification into distinct forms is being questioned because many experts believe that MS is a continuum: the inflammatory component and the degenerative component coexist from the onset of the disease, and the clinical manifestations are the result of various genetic factors, immunological factors and neurologic reserve. (Vollmer T. et al., 2021, Giovannoni et al., 2022, Kuhlmann et al., 2023).
Different Courses of MS
In this section, with respect to subtypes of MS, we summarize some of the guidelines and recommendations of scientific societies as well as position papers of experts. Each document subdivides MS in subsets that can be different or partially overlapping in comparison with other ones.
🟢 An important consensus endorses AHSCT for selected indications: “In this Consensus Statement, ECTRIMS and the EBMT, as well as lead representatives of ACTRIMS, endorse AHSCT for selected indications. In relapsing–remitting MS, AHSCT should be offered to appropriate candidates, normally after failure of high-efficacy DMT but within the window of opportunity before the development of irreversible disability.” (Muraro et al., 2025)

- France – French experts and collaborators from MATHEC (Maladies Auto-immunes et Thérapie Cellulaire) list the characteristics for undergoing HSCT in MS patients: failure at least of one highly effective treatment for at the minimum of six months. (Farge et al., 2024)
- UK – The ABN(Rashid et al., 2024) has published updated guidance on the use of DMTs in MS, supporting the appropriate use of AHSCT for treatment-resistant active inflammatory MS, in line with EBMT guidelines.
- United Arab Emirates – AHSCT is offered as second line for aggressive MS. (Jacob et al., 2024).
- Germany – This subset of pwMSis the critical for a patient to be considered for AHSCT and it has all the “core criteria” for AHSCT according the German recommendations (Bayas et al., 2023).
- Italy – Guidelines from the Italian Society of Neurology SINand theISSindicate AHSCT if no response to HE-DMT. For additional information click here and see at page 101.
 Source: ISS-Società Italiana di Neurologia SIN (2022)
Source: ISS-Società Italiana di Neurologia SIN (2022)
Australia & New Zealand: AHSCT is used selectively for younger adults (<65) with severe, treatment-resistant RRMS and lower disability (EDSS ≤6.5) who have failed at least two high-efficacy DMTs due to ongoing disease activity. (Shipley et al., 2025)
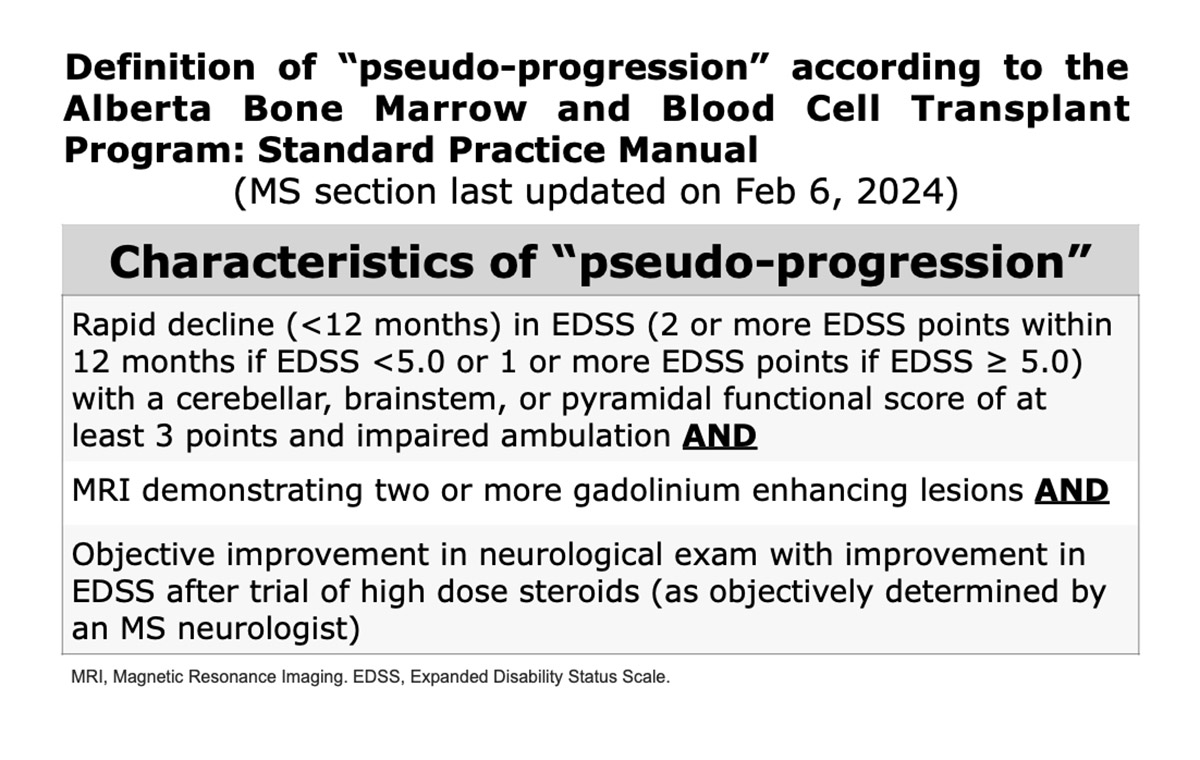
- According to the Alberta Bone and Marrow Transplant Clinic (2021), “eligibility for AHSCT includes poorly controlled RRMSor apparent pseudo-progression in highly select group of patients”. According these guidelines, “pseudo-progression” is referred to as a very active inflammatory disease. The last revision of the MS section dates back to February 6th, 2024.
🟢 A consensus on AHSCT in MS, developed by ECTRIMS, EBMT, and lead representatives of ACTRIMS (Muraro et al., 2025) recommends AHSCT for patients with highly aggressive MS and poor prognostic factors within the context of a clinical trial or study.
🟢 Recommendation of German experts (Bayas et al., 2023): “In individuals with clearly aggressive disease, AHSCT might be justified even as a first-line treatment on a case-by-case basis.”
The indications for AHSCT as a first-line treatment are rapidly evolving. Other references on this topic:
- A review on AHSCT as a first line-treatment by Mariottini et al., 2023 (“Should autologous hematopoietic stem cell transplantation be offered as a first-line disease modifying therapy to patients with multiple sclerosis?“). Click here for their review.
- For a retrospective study by Das et al., 2021 (“Autologous haematopoietic stem cell transplantation as a first-line disease-modifying therapy in patients with “aggressive” multiple sclerosis”), on 20 patients with “aggressive” MS who received AHSCT as a first-line treatment. Click here.
The Star-MS trial has enrolled patients aged between 16 and 55 with highly active RRMS. This trial has enrolled 90 patients in the study from 19 sites across the UK. Click here for more details.
- “Extended criteria” according to German recommendations (Bayas et al., 2023). See here the table for more information about the extended criteria.
- The following clinical trials are recruiting or have recruited patients with RRMS non responder to LE-DMTs. For more details: BEAT-MS, NET-MS, RAM-MS and STAR-MS.
📌 Click here for a table comparing RCTs. Click here for a detailed description of clinical trials in the “Prospective” section.
🟢 The ASBMT (Cohen et al., 2019) considers AHSCT as the “standard of care” for SPMS with high disease activity, specifically for patients who are at significant risk for progression. The ASBMT Task Force states that “The ASBMT Task Force recommends revising the recommended indication for AHCT in MS to “standard of care, clinical evidence available”, for patients with relapsing forms of MS (RRMS or progressive MS with superimposed activity) who have prognostic factors that indicate a high risk of future disability, including ongoing clinical relapse or MRI lesion activity despite treatment with available DMTs, especially if disease activity continues despite treatment with high-efficacy DMTs and/or worsening disability.”
Presented below are additional significant perspectives on this topic from various MS societies worldwide:
🟢 According to German experts (Bayas et al., 2023), a patient is suitable for AHSCT, if affected by SPMS with progression for ≤ 2 years (core criteria) or if affected by SPMS with progression ≤ 5 years (extended criteria).
In the “DMT guidelines for MS in the United Arab Emirates” (Jacob et al., 2024), AHSCT is offered as second line for aggressive MS: “Treatment naïve SPMS patients are typically begun on Siponimod or anti CD20 agents (though any drug used in RRMS can be used as per FDA). Breakthrough disease activity in the form of new MRI lesions and relapses warrants escalation to anti CD20 agents, cladribine, natalizumab, alemtuzumab, AHSCT or mitoxantrone”.
Other references on this topic:
- A study of pwMS with active secondary progressive by Boffa et al., 2022 (Hematopoietic Stem Cell Transplantation in People With Active Secondary Progressive Multiple Sclerosis). Click here.
🟢 Recommendation of German experts (Bayas et al., 2023): “Most immunotherapies do not work convincingly in PPMS; hence AHSCT should be considered with great caution.”.
They have suggested to evaluate AHSCT in selected cases of PPMS, especially if patients show inflammatory activity on MRI or relapses. “Without MRI activity, PPMS could only be considered in cases with an aggressive course, that is, EDSS 6.0 after 5 years or EDSS 6.0 before age 40 and with enhanced consideration of the benefit versus risk balance”.
🟢 According to the review by the EBMT Autoimmune Diseases (ADWP) and Paediatric Diseases (PDWP) Working Parties (2022), “Autologous and allogeneic HSCT have been used successfully to induce disease control and often apparent cure of severe treatment-refractory autoimmune diseases (ADs) in children.” (Achini-Gutzwiller et al., 2022)
In this review, the authors state that HSCT, particularly AHSCT, is considered a therapeutic option for pediatric MS cases that are refractory to conventional treatments such as interferon beta (IFN β), glatiramer acetate (GA), natalizumab, or rituximab. However, a careful assessment of the risks and benefits in a multidisciplinary setting is essential. (Achini-Gutzwiller et al., 2022)
🟢 A detailed description of pediatric MS has been developed in Chapter 15 of the Hematopoietic Stem Cell Transplantation for Neurologic Diseases, Handbook of Clinical Neurology by Elsevier (2024).
Other references on this topic:
- Read here an important study on 7 pediatric patients with AIDs treated with AHSCT, with a median follow-up of 17 years. “All patients are still alive and 4/7 are in clinical remission on medication, 3/7 in clinical remission off medication” (Satirer et al., 2024).
- A study on 21 young patients (aged 9-18) treated with AHSCT (Burman et al., 2017) reported encouraging outcomes, with 100% overall survival and progression-free survival (PFS) at three years after AHSCT.
Other Neurological AIDs
The following is a list of autoimmune diseases of both central and peripheral nervous system, on which publications have been made since 2024 to date. It is beyond the scope of this website to detail other diseases but MS.
The table lists various neurological autoimmune diseases where AHSCT has been performed, offering an overview of treated cases.
For further insights on transplant in other neurological autoimmune disorders:
- Hematopoietic Stem Cell Transplantation for Neurologic Diseases. 1st Edition, Volume 202. Handbook of Clinical Neurology. Editors: Matilde Inglese, Giovanni L. Mancardi (2024).
- Download the EBMT Handbook for free here, authored by over 200 experts and renowned authorities in the fields of HSCT and Cellular Therapies (2024).
- Read the book “Hematopoietic Stem Cell Transplantation and Cellular Therapies for Autoimmune Diseases” edited by Prof. R.K. Burt et al. (2021).