INDEX:
For Patients
EBV Vaccines
Research in MS has made significant progress in understanding the mechanisms behind the disease. In recent years, strong scientific evidence has shown that infection with Epstein–Barr Virus (EBV)—the virus that causes mononucleosis—is a necessary but not sufficient factor for developing MS. In other words, exposure to EBV appears to be a critical first step, although it is not the only cause of the disease.
For this reason, developing a vaccine against EBV is not just a way to prevent mononucleosis—a very common infection affecting around 90% of the global population—but also represents a real hope to reduce the risk of MS, improve disease management, and potentially open new strategies toward a future “cure.”
This strategy works in two ways:
- Preventing initial infection – stopping subclinical infection, mononucleosis, EBV-driven tumors, and the potential development of MS.
- Targeting latent or reactivated virus – reducing or limiting MS disease activity.
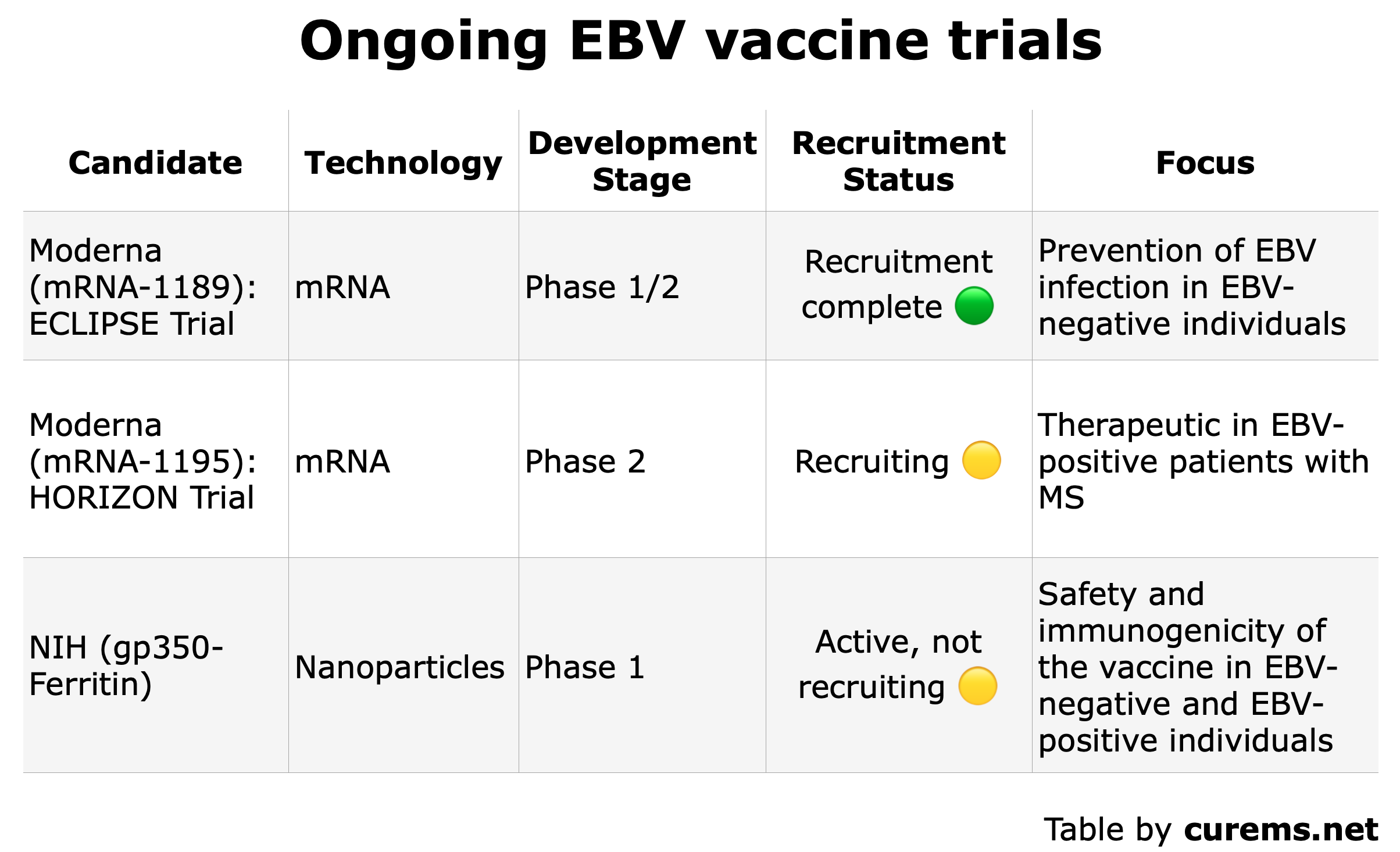
So far, many EBV vaccine candidates are being studied in the lab, and three vaccines are already being tested in people:
CAR-T Cell Therapy
CAR-T cell therapy is an immunotherapy that retrains the immune system. In the lab, scientists add a new gene into the T cells. This gene gives the cells special instructions to make a new receptor (a kind of “sensor” on the cell’s surface).
Doctors take some of your T cells, reprogram them in the lab so they can find and destroy harmful B cells, then put them back into your body. Because B cells can damage the myelin coating around nerves in MS, this treatment could help slow down or even stop disease progression.
For Healthcare Professionals
Hot Topics for Researchers
CureMS.net seeks to contribute to the scientific debate on AHSCT. This section presents research topics.
Epigenetic Rejuvenation After AHSCT in MS
Recent research suggests that AHSCT does more than just reset the immune system in aggressive MS – it may also rejuvenate the body at the molecular level.
Our DNA carries epigenetic marks that control how genes work. These marks change with age and inflammation, a process called epigenetic aging. People with MS often show accelerated epigenetic aging, especially in immune cells and brain tissue, linked to chronic immune activation and neurodegeneration.
In other diseases, such as blood cancers, studies show that after AHSCT the epigenetic “clock” temporarily turns back, making blood cells appear biologically “younger”. This likely reflects the replacement of old, defective immune cells (before AHSCT) with new ones derived from transplanted stem cells (post-AHSCT).
Why It Matters for MS
🔵 Known: MS involves epigenetic dysregulation and premature aging of immune cells (Maltby et al., 2023, Goyne et al., 2025)
🟢 Promising: AHSCT causes profound epigenetic changes in other diseases (Mohanraj et al., 2022), suggesting similar benefits may occur in MS.
🟡 Unanswered questions: How long this rejuvenation lasts and whether it predicts long-term remission remain under study.
If confirmed, epigenetic markers could become valuable tools to predict who will benefit most from AHSCT and track deep, long-lasting recovery. This research may help refine treatment strategies, aiming for not just relapse control, but durable remission and slower disease progression.
Ongoing AHSCT Trials
Clinical trials are in vivo research studies aimed at evaluating the safety, efficacy and potential adverse effects that may occur during or after transplant.
In this context, clinical trials are highly valuable tools that, over the years and with the experience gained by the AHSCT Centers, help to identify the “ideal candidate” and the “ideal window” for performing the procedure.
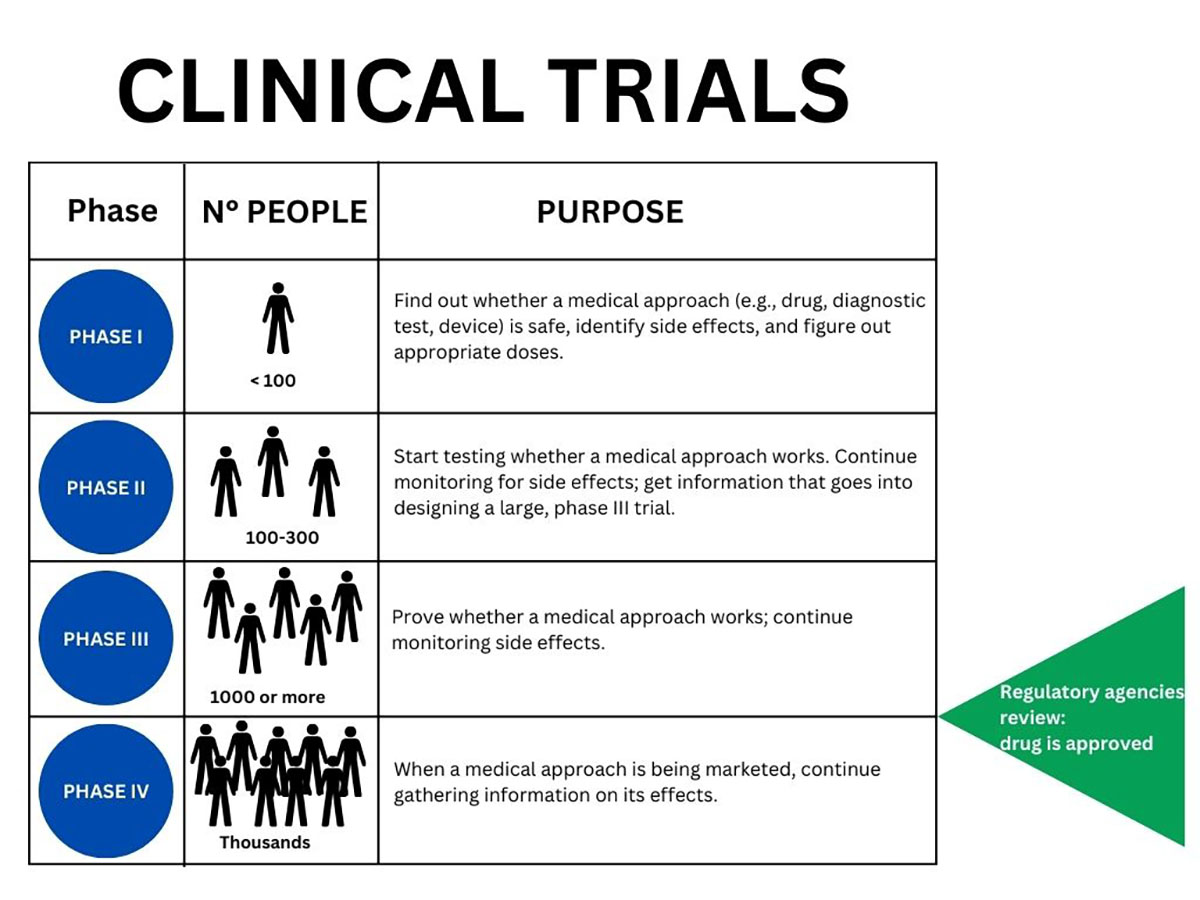
Figure created by curems.net based on an NIH (USA) infographic
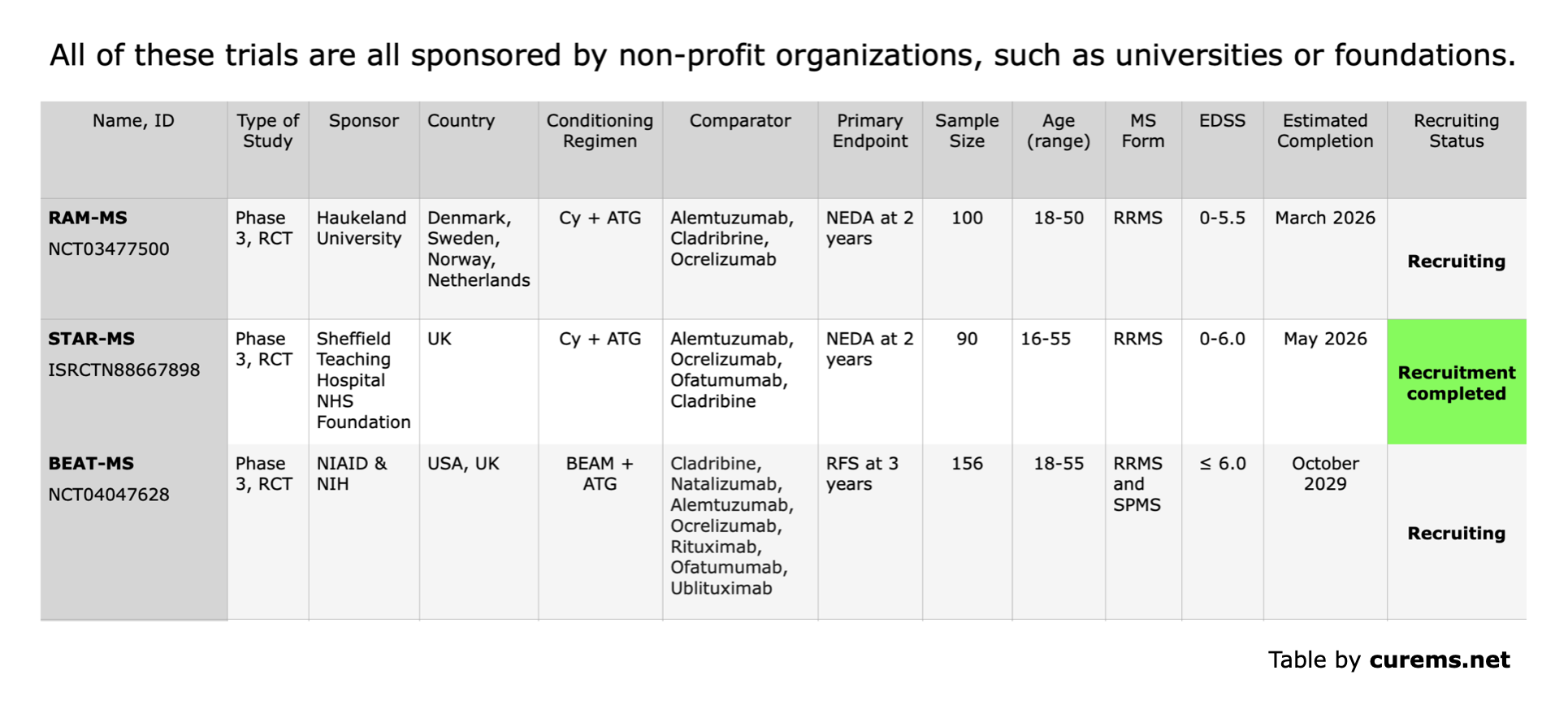
Each study is assigned a unique ID, and this website provides a link for easy access. All study reports are freely available to the public. These trials will generate important evidence to guide the use of AHSCT in the future. Their results are expected to become available over the next decade.
Ongoing Trials (Last Updated July 2026)
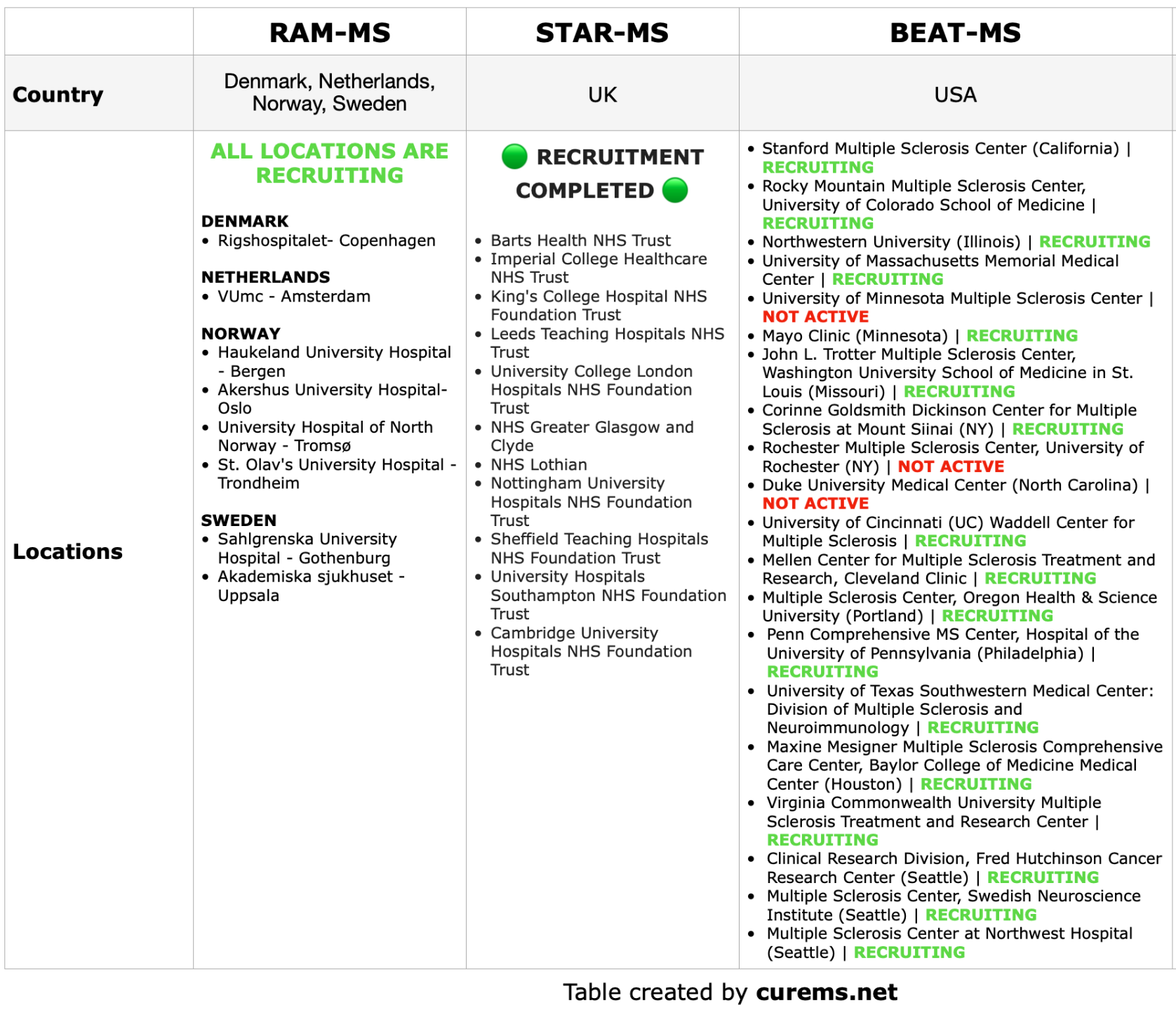
The table shows the recruiting centers involved in trials (July 2026)
RAM-MS Trial
RAM-MS trial is a phase 3 trial conducted in Scandinavia and the Netherlands, sponsored by the Haukeland University Hospital (Norway).
A pre-planned 3-year follow-up extension period will be performed depending on future funding.
The aim of the study is to assess the effectiveness and side effects of a new treatment intervention in RRMS; HSCT, and, thereby, the value of HSCT in clinical practice. Data from recently published patient series indicate that HSCT may have a significantly higher treatment effect than currently registered RRMS immunomodulatory treatments. This study will determine the relative role of HSCT versus alemtuzumab, cladribine or ocrelizumab” (from ClinicalTrials.gov).
➡️ Study details on ClinicalTrials here
📌 Contacts here
STAR-MS Trial
The StarMS trial, is a phase 3 study that recruited patients from 19 center in the UK. Star-MS is set to compare HSCT with highly potent DMTs: Alemtuzumab, Ocrelizumab, Cladribine and Ofatumumab.
This project is founded by the Efficacy and Mechanism Evaluation (EME) Programme, an MRC and NIHR partnership, and sponsored by the Sheffield Teaching Hospitals.
“Star-MS is a multicentre rater-blinded randomised controlled trial of AHSCT versus high efficacy DMT (alemtuzumab, cladribine, ocrelizumab and ofatumumab) of 90 RRMS patients in the United Kingdom (England, Scotland, United Kingdom, Wales). Haematopoietic stem cells are obtained following cyclophosphamide based priming and AHSCT is delivered using non-myeloablative conditioning with cyclophosphamide and anti-thymocyte globulin followed by an unselected autologous graft.” As of September 2024, Star-MS has recruited all 90 patients, and the recruiting is completed.
🟢 Official Website here
➡️ Study details on the International Clinical Trials Registry Platform (ICTRP) here
📌 Contacts here
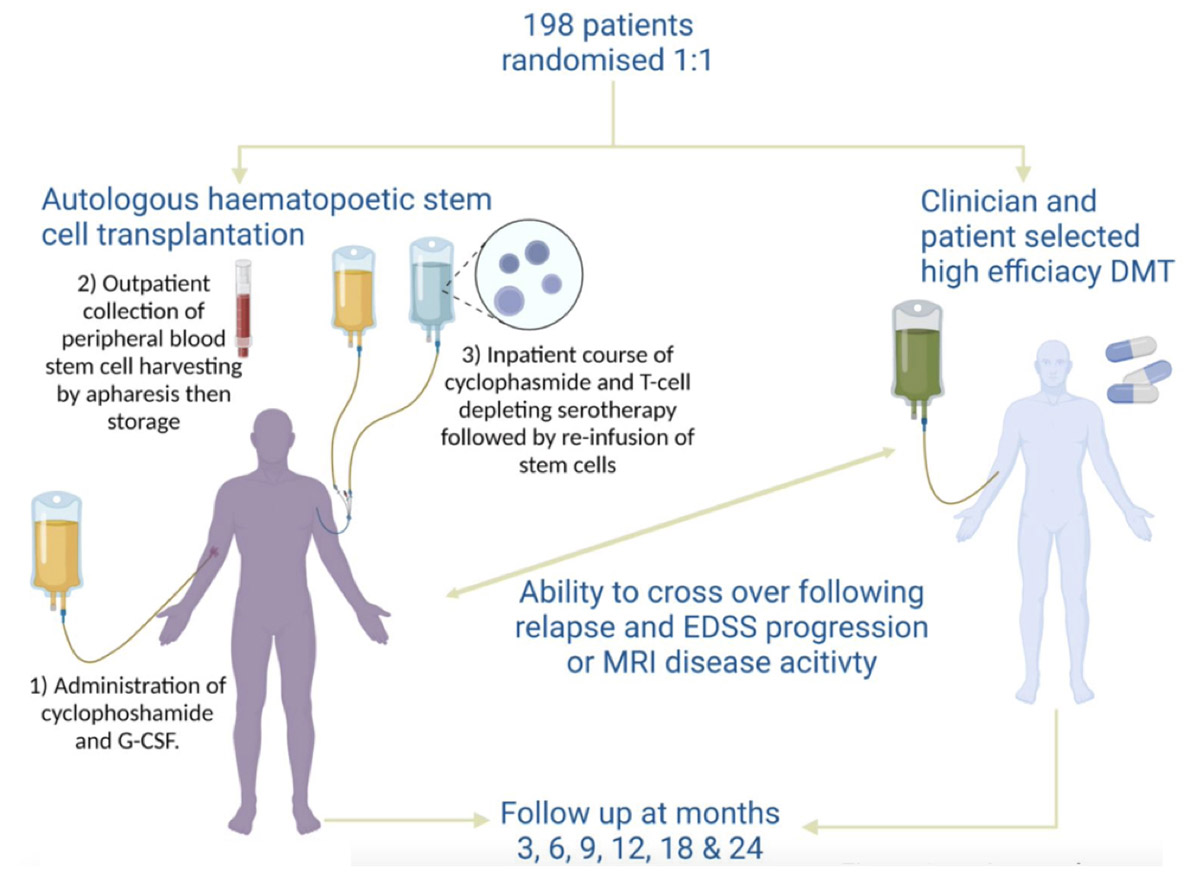
Figure from Brittain et al. “A changing target – adapting autologous haematopoietic stem cell transplantation clinical trials to evolving clinical practice in highly active relapsing remitting multiple sclerosis”. Star-MS Trial poster at ECTRIMS 2022.
It is important to note that the figure above represented the initial enrollment numbers required by the trial. This number was later reduced based on statistical evaluations (personal communication at ECTRIMS 2024). As of September 2024, STAR-MS has successfully recruited all 90 participants.
Two randomized clinical trials are comparing AHSCT (BEAM + ATG) against a range of high-efficacy DMTs representing the best standard care:
BEAT-MS Trial
This study has 19 locations. BEAT-MS is sponsored by the National Institute of Allergy and Infectious Diseases and conducted in collaboration with the Immune Tolerance Network in the US and UK. The researchers will monitor the patients for a duration of 6 years, with an anticipated study conclusion in 2029.
🟢 Official website here
➡️ Study details on ClinicalTrials here
📌 Contacts here
Other Hopes to Cure
EBV Vaccines
This approach aims either to prevent Epstein–Barr virus (EBV) infection in individuals who are EBV-negative or to block EBV-driven immune activation in those who are already EBV-positive. EBV infection has been identified as a necessary but not sufficient factor for the development of MS (Bjornevik et al., 2022). Preventing infection—or modulating its downstream effects—could potentially reduce/abolish the risk of MS or influence disease activity.
One of the leading proponents of this hypothesis is Professor Giovannoni, who has shown sustained interest in this area and has published extensively on EBV and its role in MS (Giovannoni G., 2024).
The race to develop the first approved vaccine for the EBV is challenging, with three main candidates and several other studies in preclinical phase currently in development across different clinical stages.
These trials and studies are exploring different technologies (like mRNA and nanoparticles) and approaches, with the goal of:
- Preventing Initial Infection (subclinical infection, mononucleosis, EBV-induced tumors, and development of MS);
- Targeting Latent/Reactivated Virus (riduce/abolish the MS activity).
To date, five different EBV vaccine candidates are currently in the preclinical phase, exploring multiple approaches (Dai et al. “Recent Progress in the Vaccine Development Against Epstein–Barr Virus“. Viruses, 2025):
Several EBV vaccine candidates have been developed and evaluated at the preclinical stage, and some reached early clinical trials (Phase I or II); however, none have advanced to late-stage clinical development to date (Dai et al. “Recent Progress in the Vaccine Development Against Epstein–Barr Virus“. Viruses, 2025):
CAR-T Cell Therapy
Another approach that potentially could lead to a cure for MS, utilizes CAR-T cells. These cells which target CD-19 lymphocytes or plasma cells via B-cell maturation antigen (BCMA) have demonstrated remarkable efficacy in treating leukemia, lymphoma, multiple myeloma, and autoimmune diseases (Baker et al., 2024).
This topic is still in its early stages, and time will be needed to determine the timelines, benefits, and risks. It is a subject of intense scientific debate.
🟢 The first two cases of MS treated with CAR-T therapy (Fischbach et al., 2024) – click here to learn more.
Structural Evolution of CAR-T Receptors
All CAR-T receptors have a part that recognizes the target antigen on the diseased cell (antigen-binding domain, in dark blue). This part is connected to a structure that spans the cell membrane (transmembrane domain TMD, in light blue) and an internal component that activates the T cell (CD3ζ, in red).
More advanced CAR-T versions include extra activation domains (such as CD28, 4-1BB, OX40) that make the T cell response stronger and longer-lasting.
Some next-generation CAR-T therapies also feature cytokine signaling modules (in purple) that enhance the T cells’ ability to fight disease for extended periods.
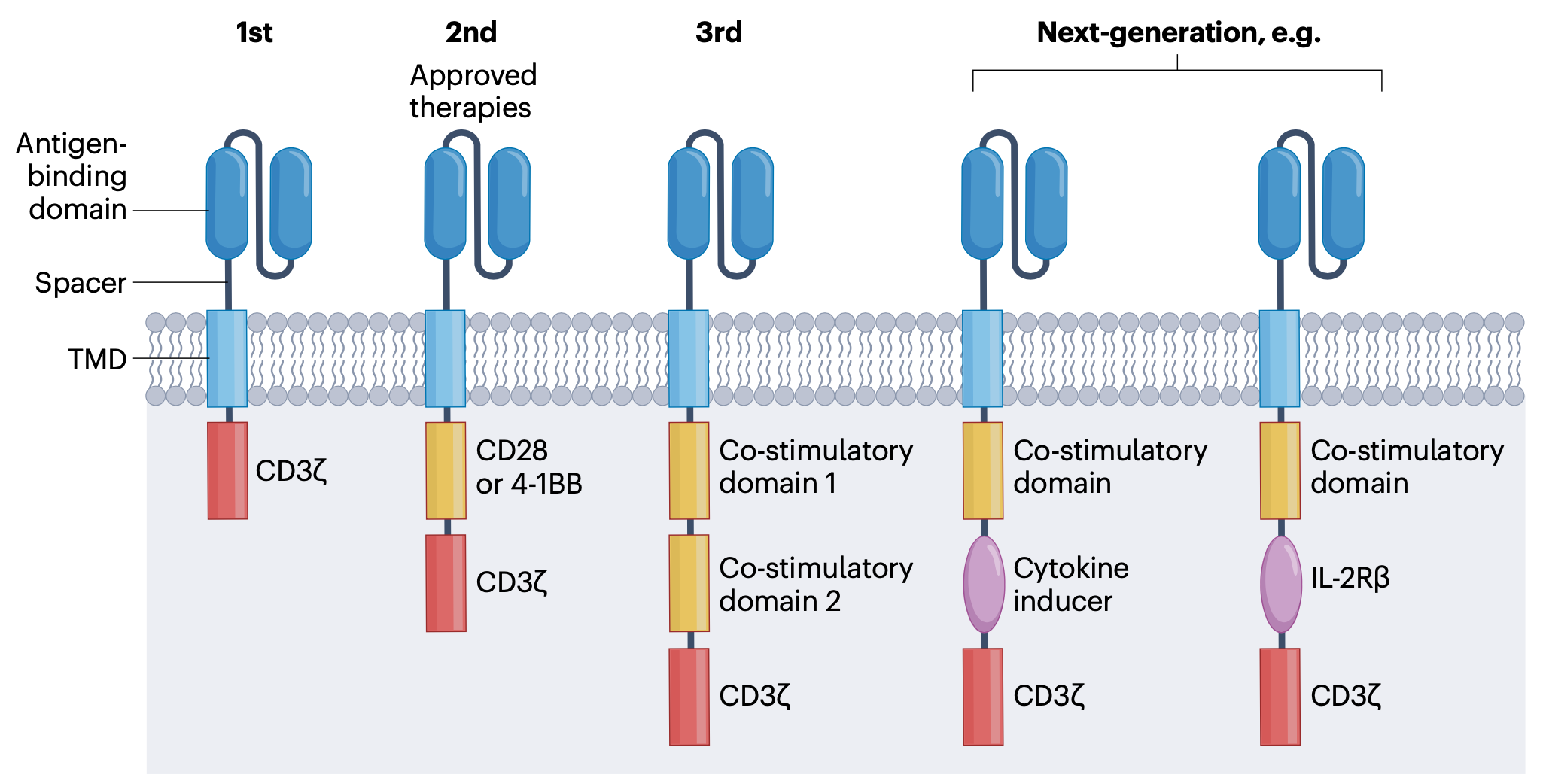
Figure from Junt et al. “Defining immune reset: achieving sustained remission in autoimmune diseases“. Nature Reviews Immunology (2025)
For further information, we recommend the following sources:
- Junt et al., 2025 “Defining immune reset: achieving sustained remission in autoimmune diseases”. Nature Reviews Immunology
- An insightful review on Neuroimmunology of Cell Therapies for Neurologic Disease, click here.
- CAR-T therapies are discussed in a popular science version on Wikipedia
- For scientific review about CAR-T and autoimmune diseases, see these reviews: Baker et al., 2024 | De Marco et al., 2023
- Promising results in an 18-year-old man with refractory MOGAD treated with CD19-directed CAR-T cells produced in-house: click here
- For secondary T-cell malignancies in patients who have received CAR-T therapy, please see the note here (for the FDA) or here (for the EMA).
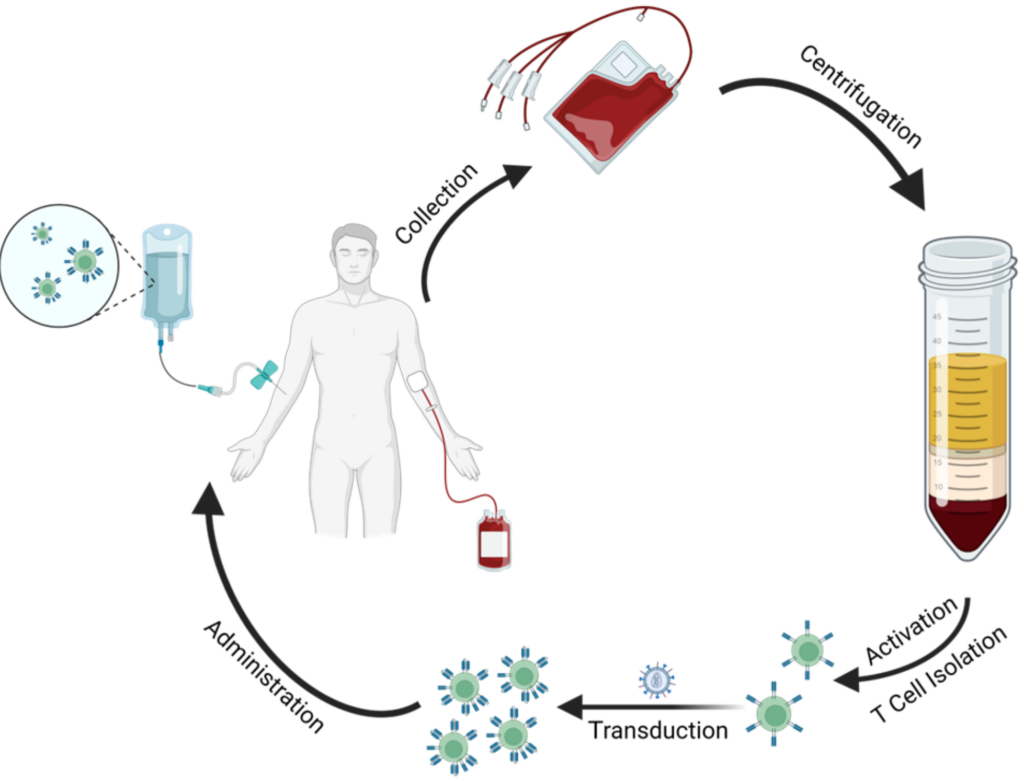
Figure from De Marco et al. “CAR T Cell Therapy: A Versatile Living Drug“. Int. J. Mol. Sci. (2023) Simplified visualization of the steps involved in an example manufacturing process for CAR-T cells.
Regulatory T Cells
In this insightful review by Ransohoff Richard M. (“Selected Aspects of the Neuroimmunology of Cell Therapies for Neurologic Disease“. Neurology. 2024), Tregs are presented as a potential therapeutic avenue for treating MS: “A distinctly different cell therapy approach for autoimmunity is to restore immune and tissue homeostasis using engineered regulatory T cells (Tregs)”.
While research is still ongoing, the idea behind using T-reg cells is based on their ability to modulate the immune system (i.e., decrease autoimmunity) and reduce the inflammatory processes that lead to demyelination and neurodegeneration in MS.
T Cell Engagers
TCEs (T-cell engagers) are a class of immunotherapeutic drugs designed to redirect a patient’s T cells to specifically target and kill other cells, such as cancer cells or, in the context of autoimmune diseases, autoreactive immune cells.
They are typically bispecific antibodies, meaning they have two distinct binding sites: one that attaches to a specific molecule (antigen) on the surface of a target cell (such as a cancer cell), and another that binds to CD3, a molecule on the surface of T cells that is part of the T cell receptor complex involved in activation.
TCEs have been primarily studied and utilized in cancer immunotherapy, enhancing the immune system’s ability to attack cancer cells. However, their potential application in autoimmune diseases like multiple sclerosis (MS) is an emerging area of research. In this context, TCEs could be designed to target and eliminate autoreactive immune cells, which are responsible for attacking the body’s own tissues in diseases like MS.
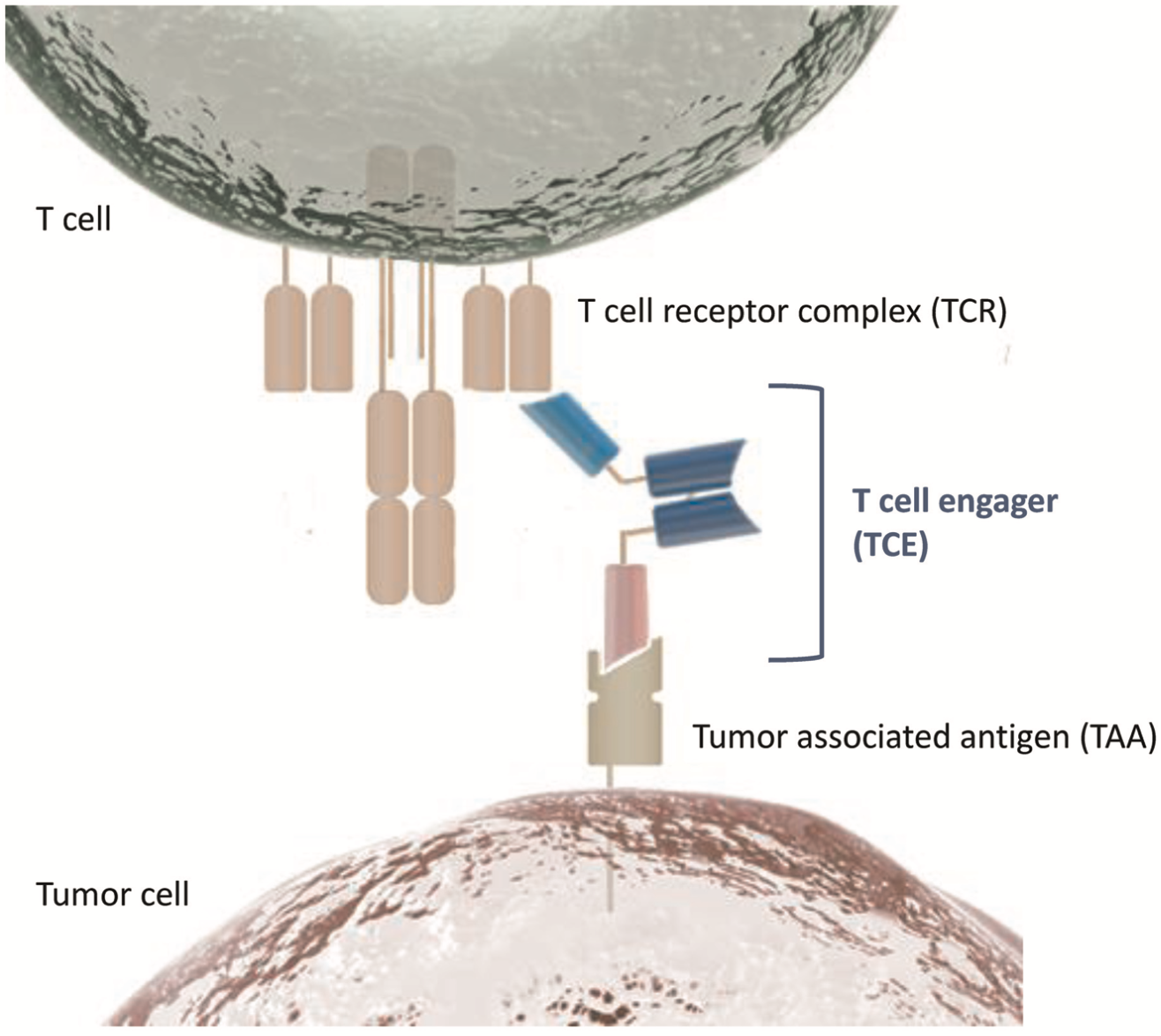
Figure from Baeuerle et al. “T-cell-engaging antibodies for the treatment of solid tumors: challenges and opportunities“. Curr Opin Oncol (2022).
T-cell engagers (TCEs) are treatments that help T cells attack cancer cells. They usually have three parts: one part attaches to the T cell, another part sticks to the cancer cell, and the third part helps the treatment last longer in the body.
Further reading: Shah et al. “Disrupting B and T-cell collaboration in autoimmune disease:T-cell engagers versus CART-cell therapy?“. Clin Exp Immunol (2024)