Clinical Evidences
Tools
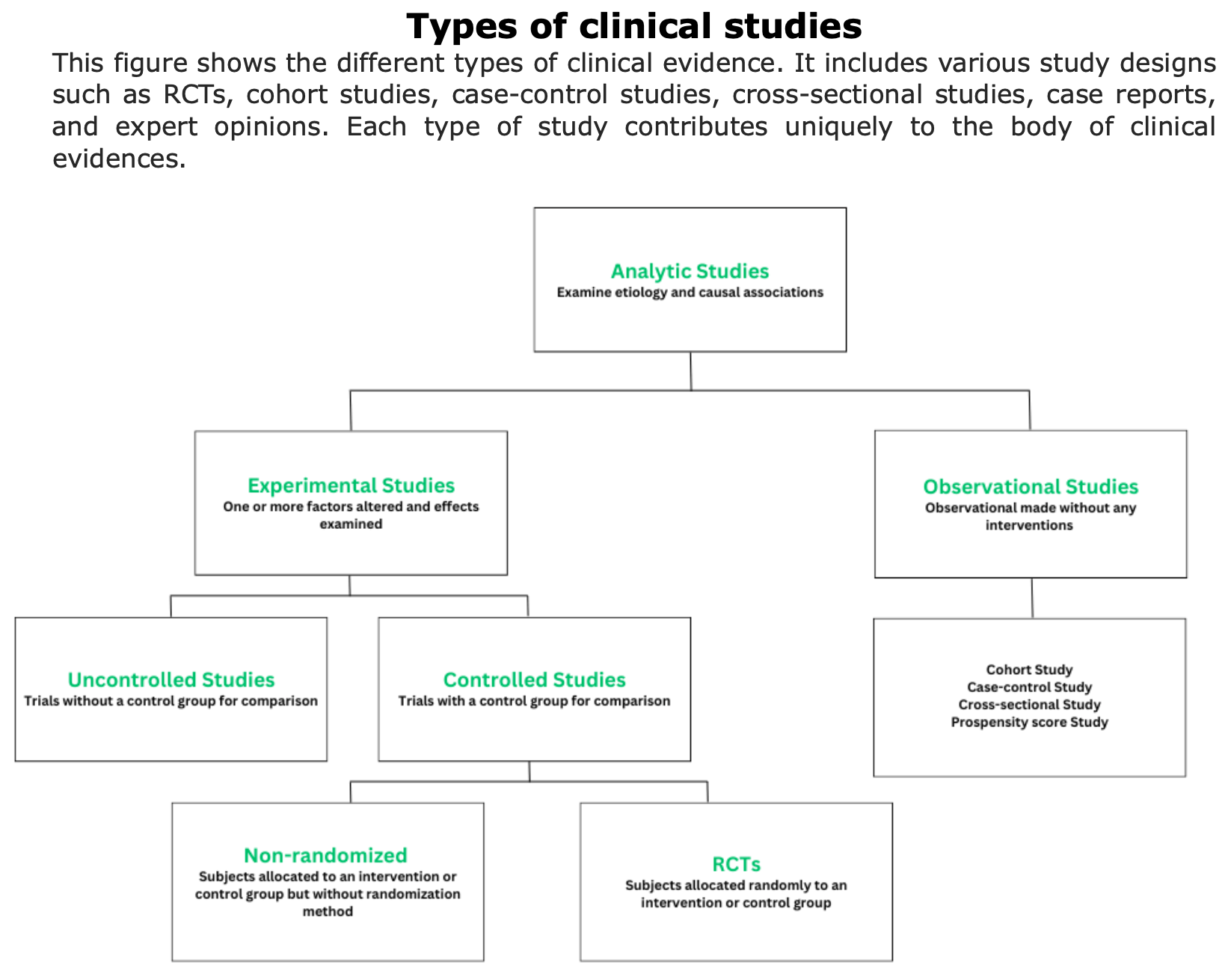
Clinical evidences are information and data collected through scientific studies and clinical observations that demonstrate the efficacy, safety, and effectiveness of treatments or procedures.
To obtain clinical evidences, various types of studies are conducted (e.g., randomized controlled trials, cohort studies, case-control studies, etc.). Each of these studies provides evidence of different strengths.
Click on these links for additional informational about how clinical evidences are collected, phases of clinical trials or class of evidences (Source: Neurology).
What are the indicators used to measure clinical evidence in MS?
To assess clinical evidences in MS field, NEDA-3, relapse-rate, EDSS score, QoL, and radiological data as valuable indicators.
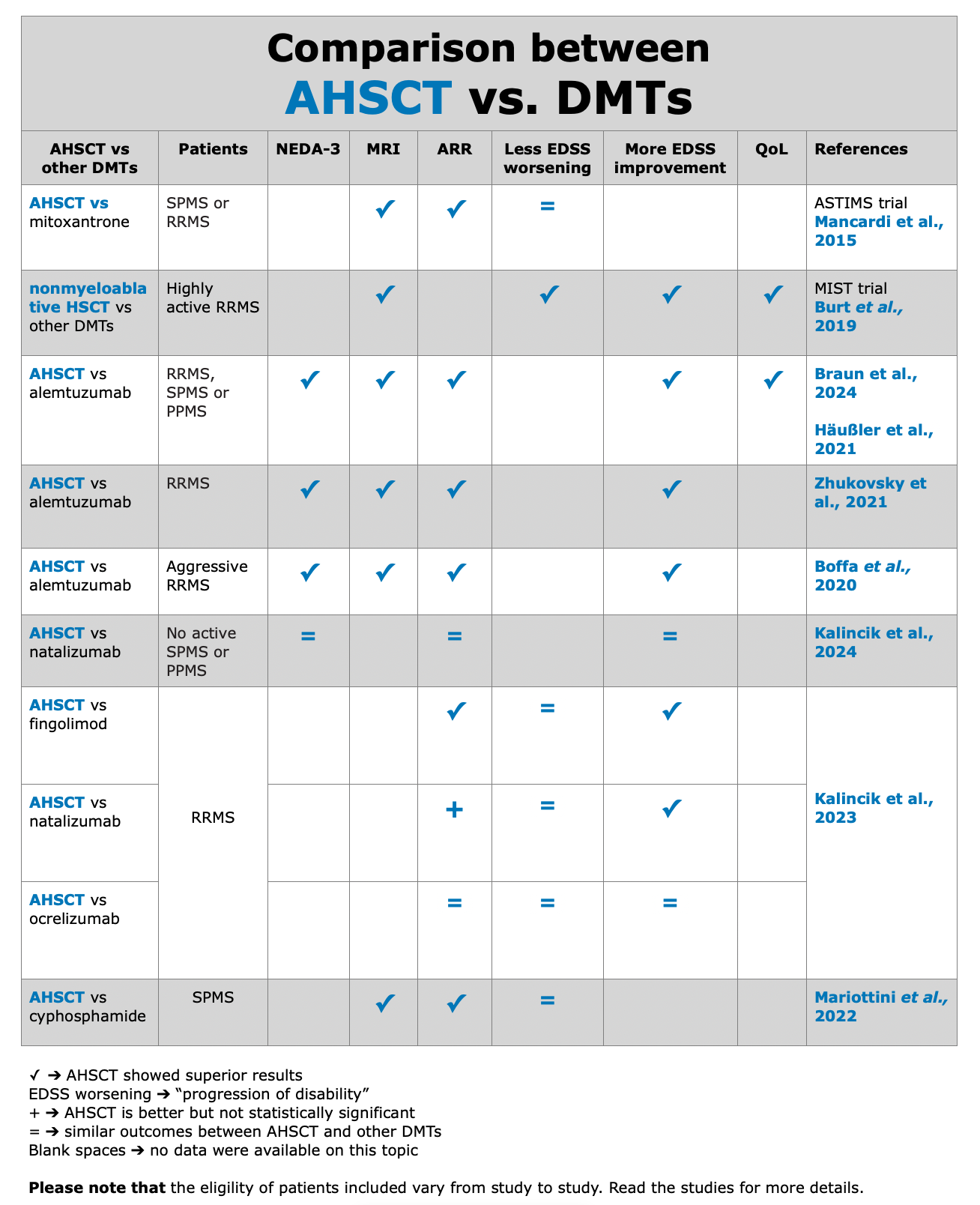
The analysis of the results shows that no treatment, in any study, has been proven to be more effective, radiologically, clinically, immunologically, and pharmaco-economically, than AHSCT (i.e., transplant).
In the following table, we include the studies comparing AHSCT vs other DMTs.
RCTs
Definition according to “A Dictionary of Epidemiology” (Miguel Porta, 2014):
RCTs completed
with published data
Below, the table that summarizes ASTIMS and MIST trial.
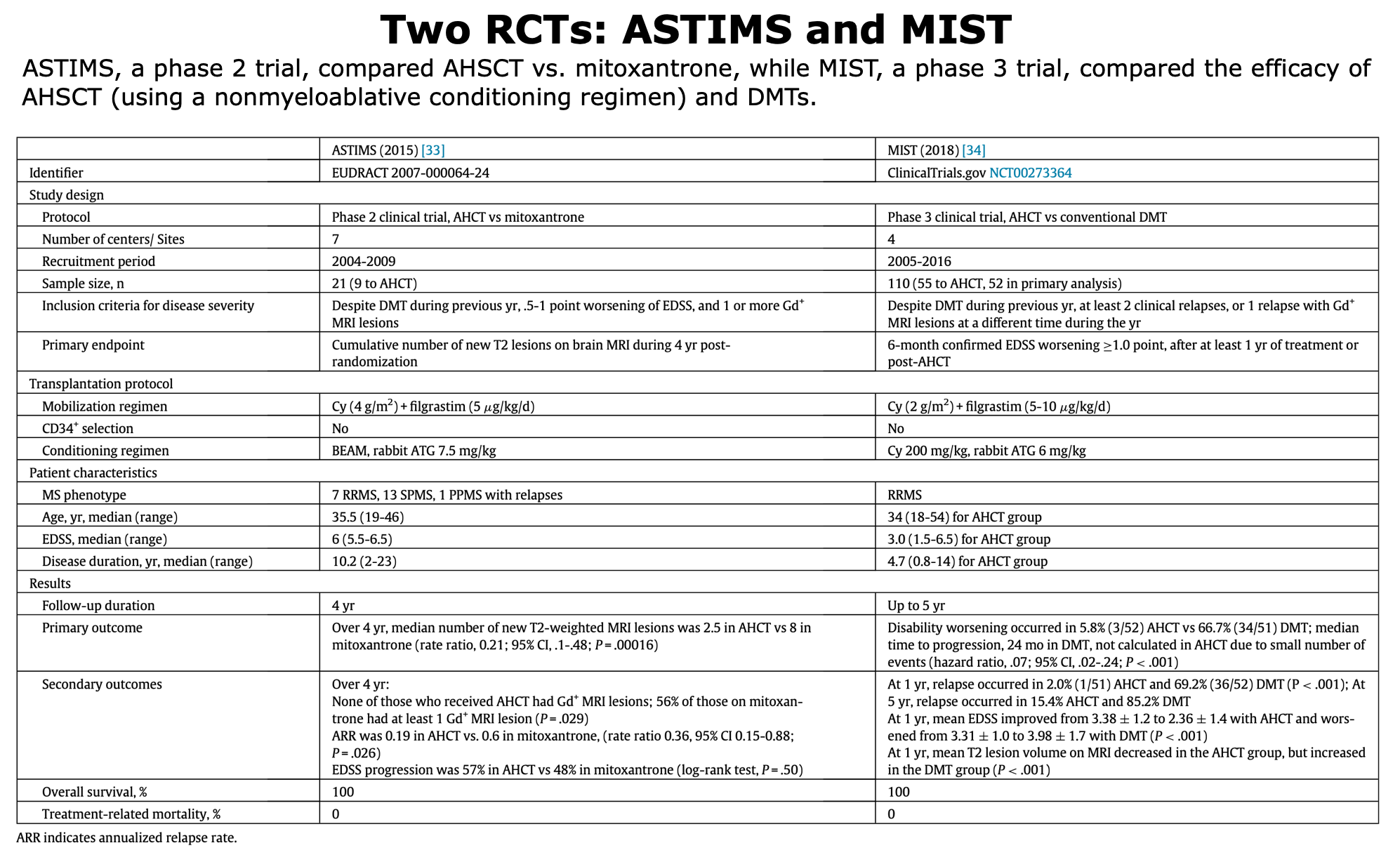
Table from Cohen et al. “Autologous Hematopoietic Cell Transplantation for Treatment-Refractory Relapsing Multiple Sclerosis: Position Statement from the American Society for Blood and Marrow Transplantation”. Biol Blood Marrow Transplant (2019).
Mancardi et al., 2015 “Autologous hematopoietic stem cell transplantation in multiple sclerosis. A phase II trial”. Neurology
This study evaluated the activity of AHSCT vs mitoxantrone on MRI measures in MS. “AHSCTT was shown to be significantly superior to MTX in reducing the MRI activity: patients in the AHSCT arm experienced 79% fewer new T2 lesions as compared to patients in the MTX arm” (Mancardi et al., 2015).
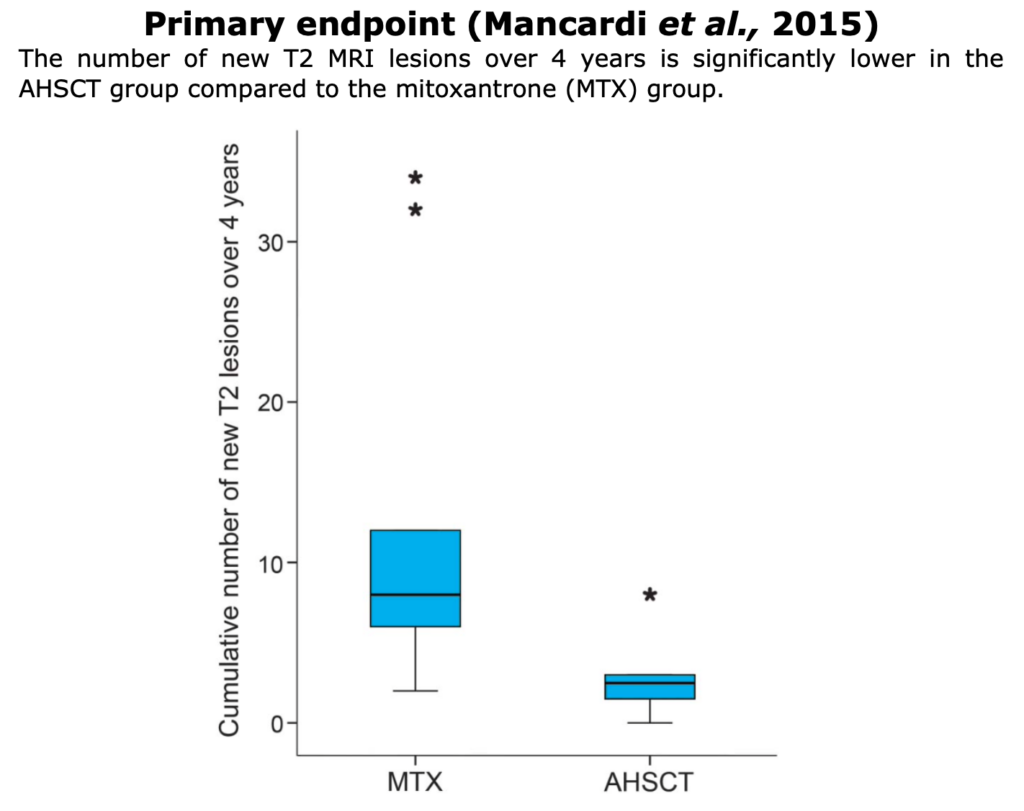
Figure from Mancardi et al. “Autologous hematopoietic stem cell transplantation in multiple sclerosis A phase II trial”. Neurology (2015).
Burt et al., 2019 “Effect of Nonmyeloablative Hematopoietic Stem Cell Transplantation vs Continued Disease-Modifying Therapy on Disease Progression in Patients With Relapsing-Remitting Multiple Sclerosis. A Randomized Clinical Trial”. JAMA
This trial was conducted at 4 centers (Chicago- USA, Sheffield- England, Uppsala- Sweden, Ribeirão Preto- Brazil) and patients were enrolled between 2005 and 2016. The main inclusion criteria were RRMS and age 18-55. This was the first randomized trial of HSCT in patients with only RRMS.
For more details about the MIST trial inclusion criteria, see the table above. For detailed information about the trial, click here.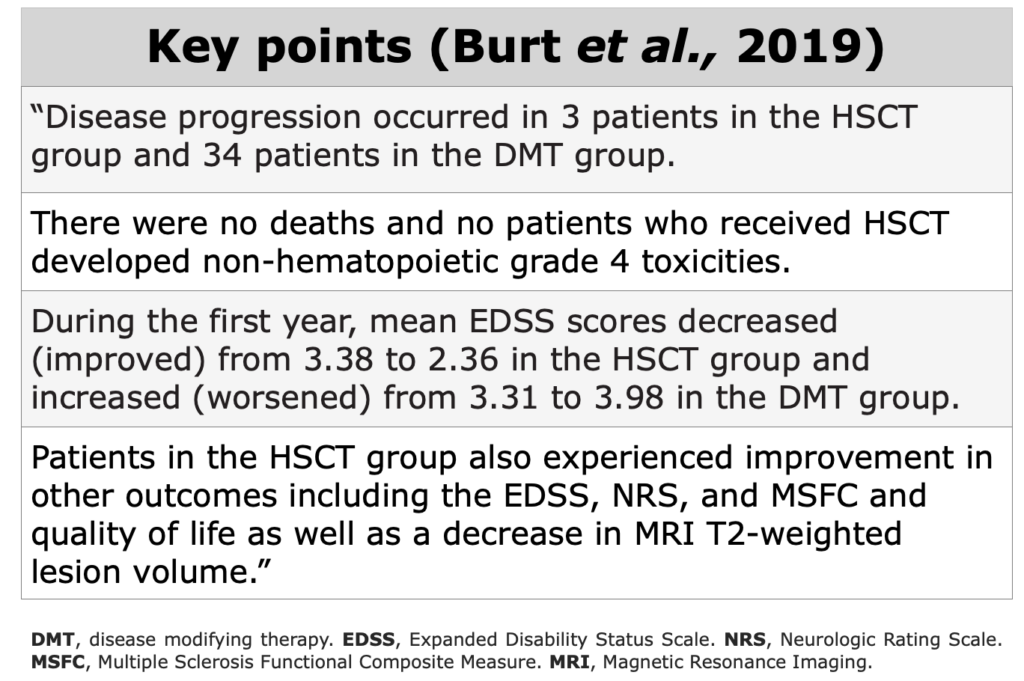
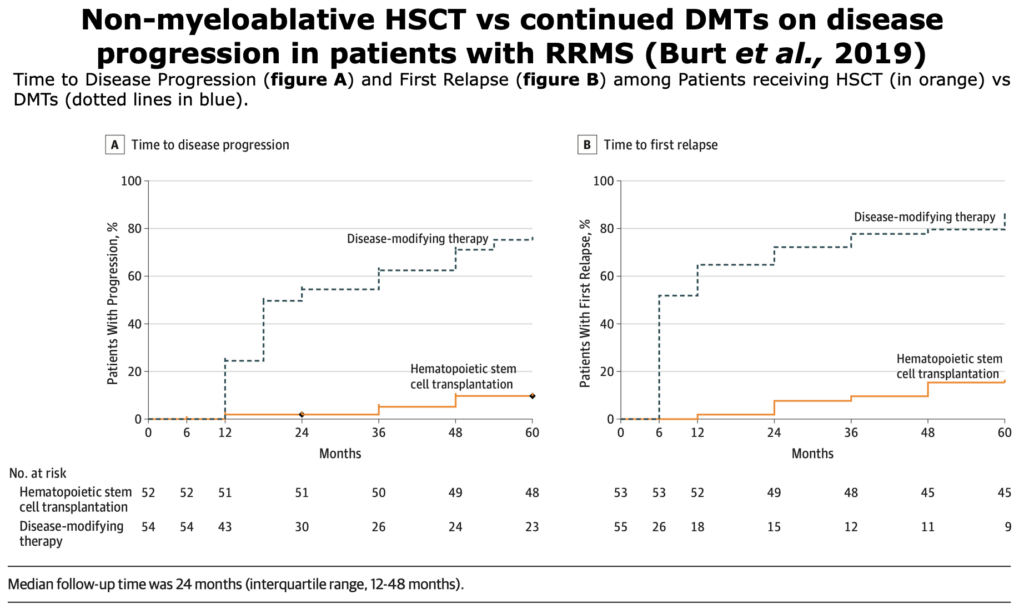
Figure from Burt et al. “Effect of Nonmyeloablative Hematopoietic Stem Cell Transplantation vs Continued Disease-Modifying Therapy on Disease Progression in Patients With Relapsing-Remitting Multiple Sclerosis. A Randomized Clinical Trial. American Medical Association”. JAMA (2019)
Limitations of this trial: the small number of patients were treated compared to pharmaceutical-sponsored trials. This smaller sample size led to a limited number of patients available for assessing long-term outcomes. In this trial were excluded ocrelizumab and alemtuzumab. Ocrelizumab was excluded because it was not FDA licensed until 2017 and the trial’s last enrollment was in 2016. According to the authors “Alemtuzumab was excluded because prolonged alemtuzumab-induced lymphopenias and secondary autoimmune disorders could contribute to or cause post-HSCT infections or autoimmune diseases in the crossover group.” (Burt et al., 2019).
RCTs - Ongoing Trials
To date, there are 4 ongoing trials. For more information, please visit the following links: BEAT-MS, NET-MS, RAM-MS trial and STAR-MS.
For the section dedicated to trials on this website, click here and here for an overview.
RCTs - Terminated
In the course of scientific research, the publication of trial results is a crucial step in advancing our knowledge. However, not all trials reach the publication stage due to challenges in recruiting, data collection, unexpected outcomes, methodological issues, or shifts in research focus.
Here we present two trials that were not published. The COAST TRIAL was terminated due to lack of recruitment caused by low acceptance of the control arm, while the MOST trial was terminated due to sabbatical principal investigator.
Observational Studies
In observational studies, researchers do not assign participants to get an intervention. If there is an intervention, participants were already using it as part of their regular health care or daily life”. The main limitation in these types of studies is that they are not randomized.
Observational Prospective Studies
Observational prospective studies follow a group of individuals over time to track their exposure to certain factors and health outcomes. Researchers analyze the relationship between exposures and outcomes to identify potential health risks.
Braun et al., 2024. “Benefits of AHSCT over alemtuzumab in patients with multiple sclerosis besides disability and relapses: Sustained improvement in cognition and quality of life”. Multiple Sclerosis and Related Disorders
This monocentric study provides an update of the data published in 2021 by Häußler et al.
Braun et al., 2024 studied 20 AHSCT-treated patients and 21 patients treated with alemtuzumab between 2007 and 2020. The most recent patient was included in 2020. This was a study compared long-term QoL, cognitive function, and fatigue.
The authors “underline the long-term effectiveness of transplant in the treatment of MS, with the potential to improve disability, especially neuropsychological functioning, and preserve QoL” (Braun et al., 2024)

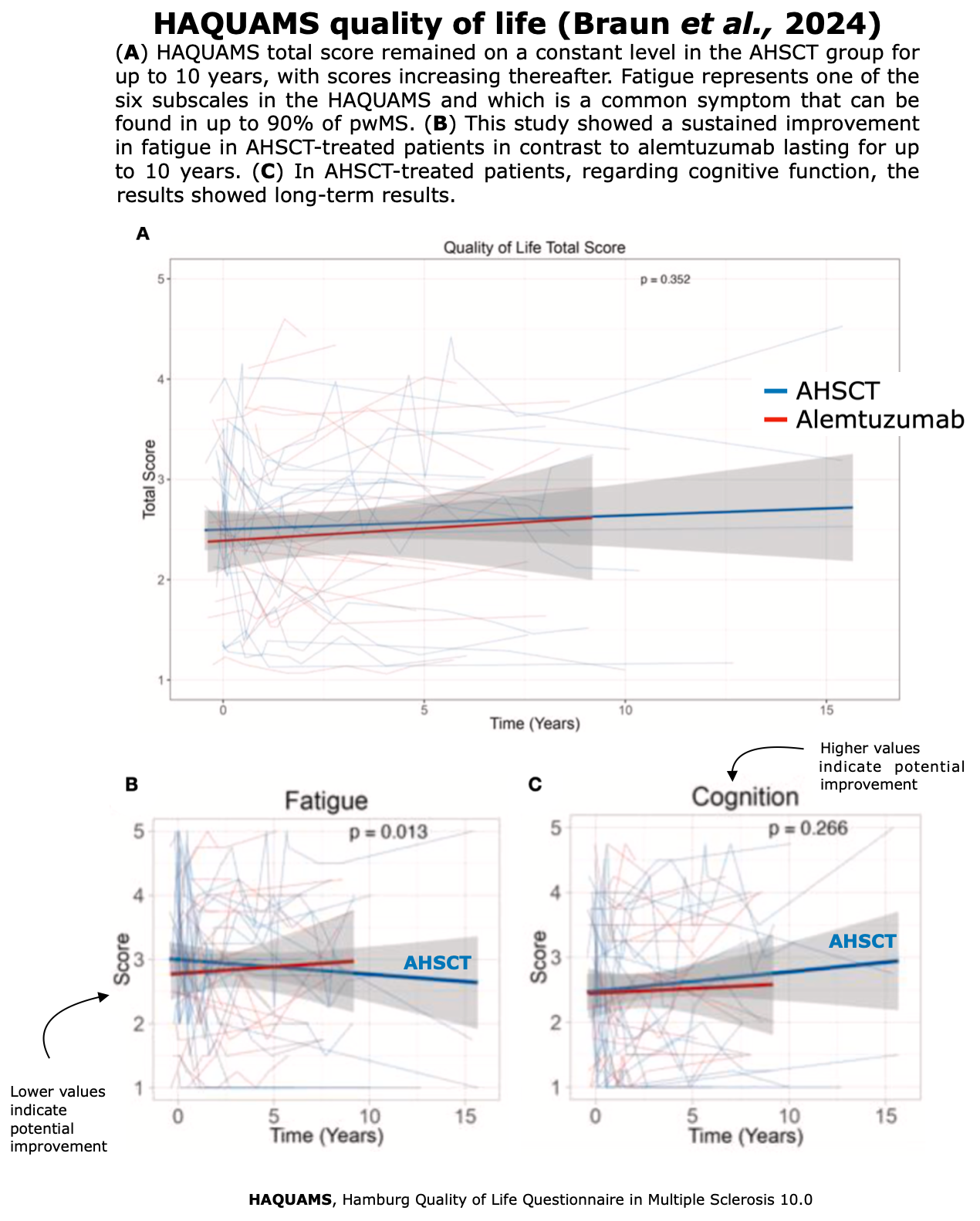 Figures from Braun et al. “Benefits of AHSCT over alemtuzumab in patients with multiple sclerosis besides disability and relapses: Sustained improvement in cognition and quality of life”. Multiple Sclerosis and Related Disorders (2024)
Figures from Braun et al. “Benefits of AHSCT over alemtuzumab in patients with multiple sclerosis besides disability and relapses: Sustained improvement in cognition and quality of life”. Multiple Sclerosis and Related Disorders (2024)
Limitation: The main limitation was the small size sample (41 patients: 20 AHSCT + 21 treated with alemtuzumab) and, again the non-randomized design.
Finally, the follow up among the two groups (AHSCT vs alemtuzumab) was different. AHSCT group did a 3 year longer follow up.
Burt et al., 2022 “Real‐world application of autologous hematopoietic stem cell transplantation in 507 patients with multiple sclerosis”. Journal of Neurology.
This is observational study of prospectively collected data on 511 patients (414 with RRMS and 93 with SPMS) who underwent AHSCT at Northwestern University (USA) between July 2003 and October 2019. Unlike DMT trials, patients had received a mean/median of 4 prior DMTs before AHSCT and 2 out of 511 patients underwent prior AHSCT. The median follow up was 5 years.
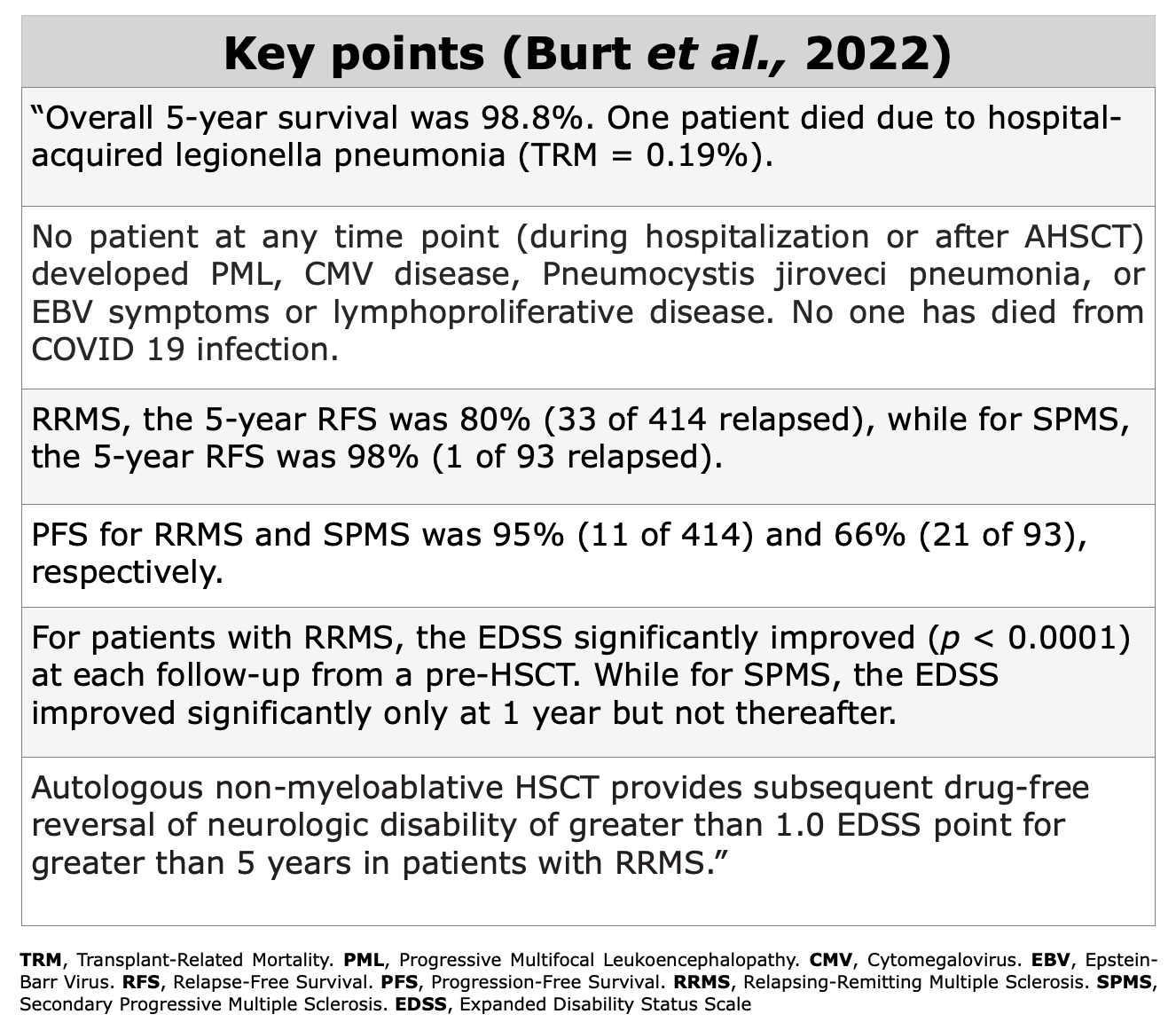

Figure from Burt et al. “Real‐world application of autologous hematopoietic stem cell transplantation in 507 patients with multiple sclerosis”. Journal of Neurology (2022)
This study included 40 patients: 19 MS patients received AHSCT, and all 21 patients were treated with alemtuzumab between 2007 and 2018 at the University Medical Center Hamburg-Eppendorf, Germany.
Among AHSCT-treated patients: there were 12 with RRMS, 3 with PPMS and 4 with SPMS In contrast, alemtuzumab-treated patients were predominantly RRMS (16 patients) and only 5 were classified as SPMS.
“We used survival analyses of NEDA as the primary objective which was defined by no EDSS progression, no relapse, and no new T2 lesion on MRI. Secondary objectives were EDSS improvement and neurocognitive performance” as reported by Häußler et al.
As indicated in the study “AHSCT suppresses inflammatory activity more effectively than alemtuzumab and might enable improvement of overall disability and cognition in MS” Häußler et al.
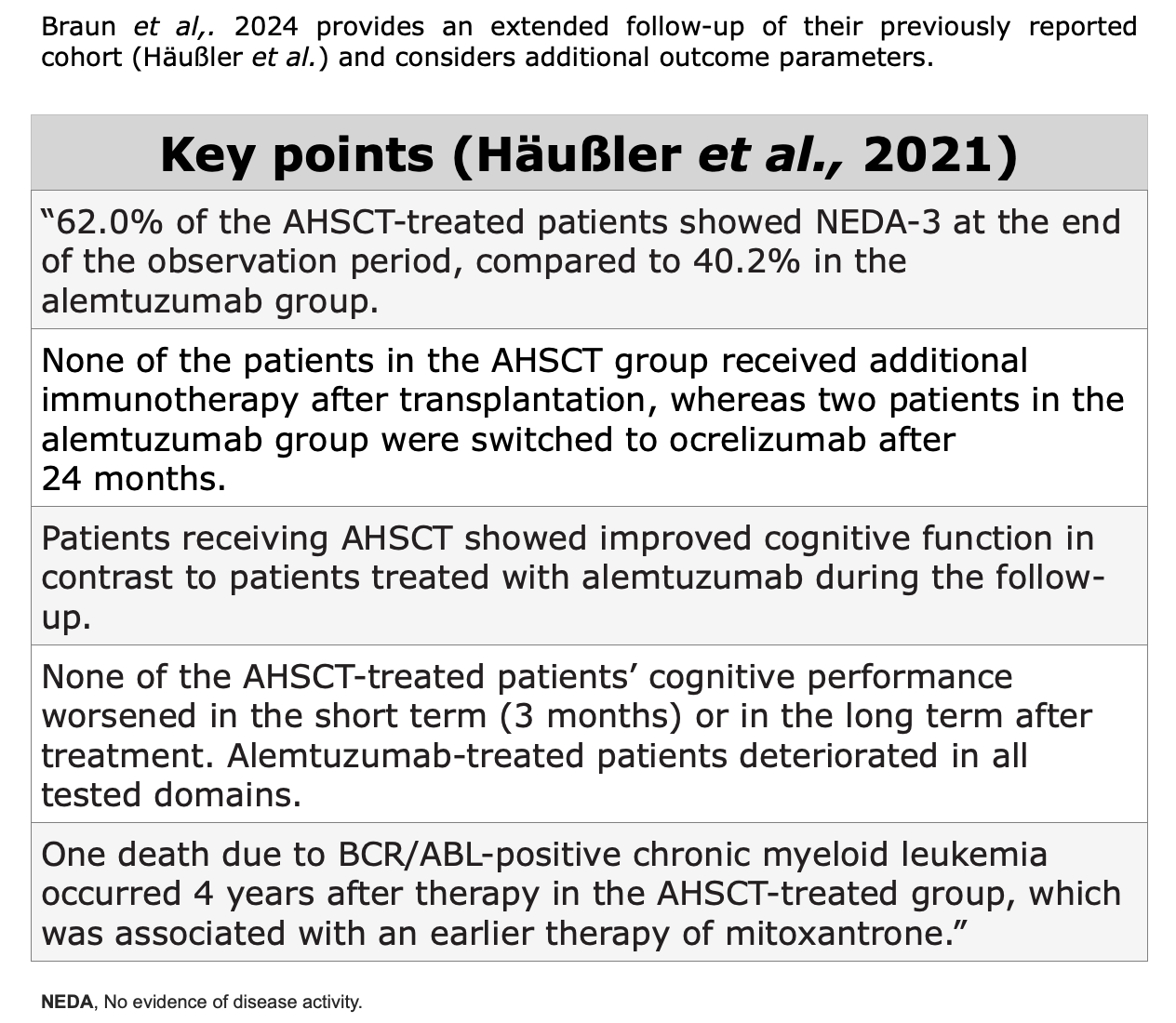
Figure from Häußler et al. “AHSCT is superior to alemtuzumab in maintaining NEDA and improving cognition in multiple sclerosis”. Annals of Clinical and Translational Neurology (2021)
Limitation of this study: Small size sample, non-randomized. “Additionally, relapses cannot always be assessed objectively and the EDSS is known to have a poor inter-rater validity” (Häußler et al.)
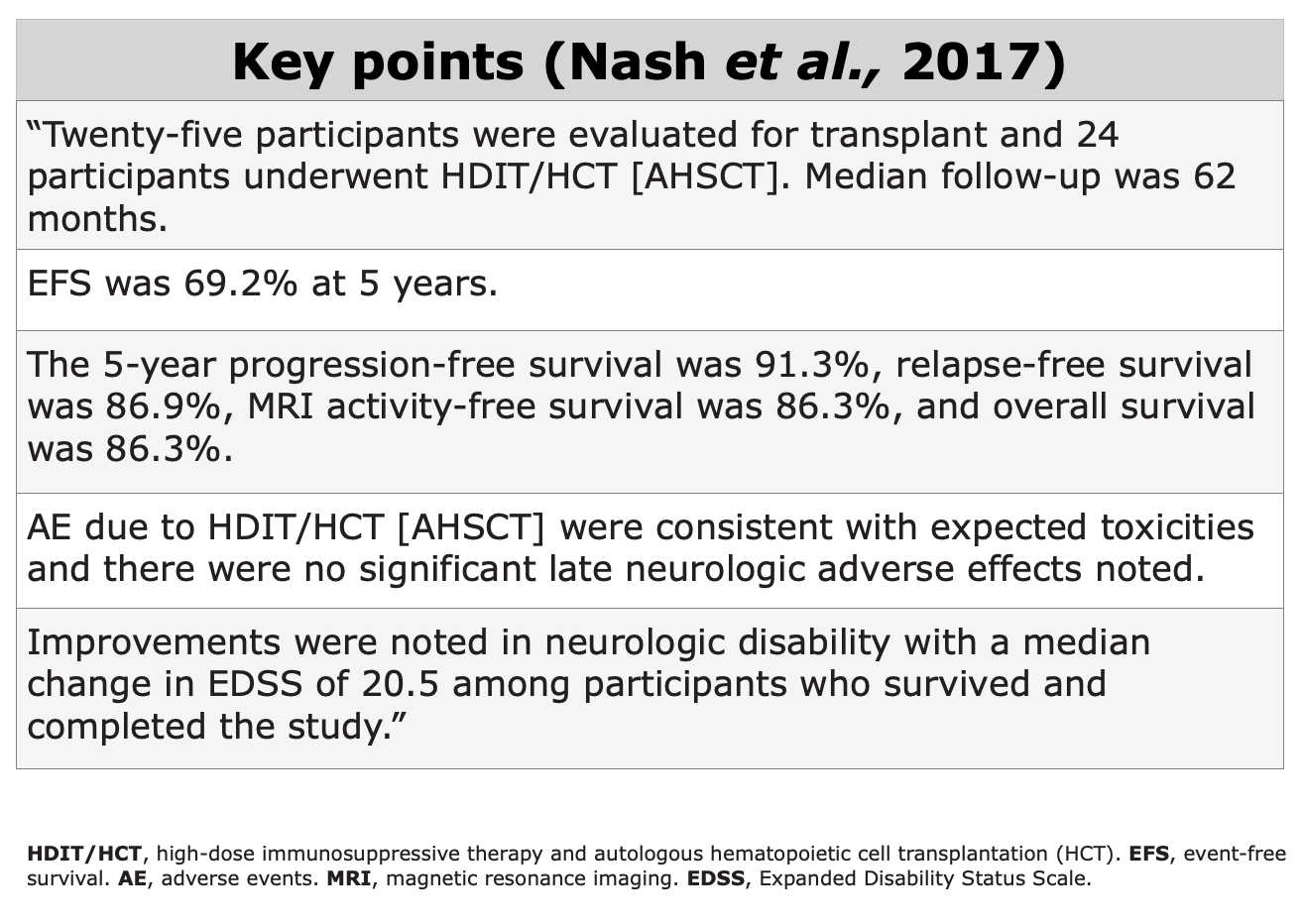
Aim: “To evaluate the safety, efficacy, and durability of MS disease stabilization after high-dose immunosuppressive therapy (HDIT) and autologous hematopoietic cell transplantation (HCT).” Nash et al., 2017
In this study, which provided Class IV evidence, were included patients with highly active RRMS. EDSS at baseline was 4.5. Participants had previously a median of failed 3 DMTs. The study followed outcomes for at least 5 years.
“The primary end-point was time until treatment failure or EFS during 5 years post-HCT, defined as the first event of death or disease activity from any one of: (1) disability progression, (2) relapse, or (3) new lesions on MRI” Nash et al., 2017.
AEs recorded at 4 and 5 years post-transplant were unrelated to the procedure and generally not severe. Two reported deaths occurred later, at over 2.5 and 3.5 years post-AHSCT. A third death occurred at 4.5 years due to cardiorespiratory arrest. “These participants had all experienced worsening of MS, and no death was related to the study treatment.” Nash et al., 2017.
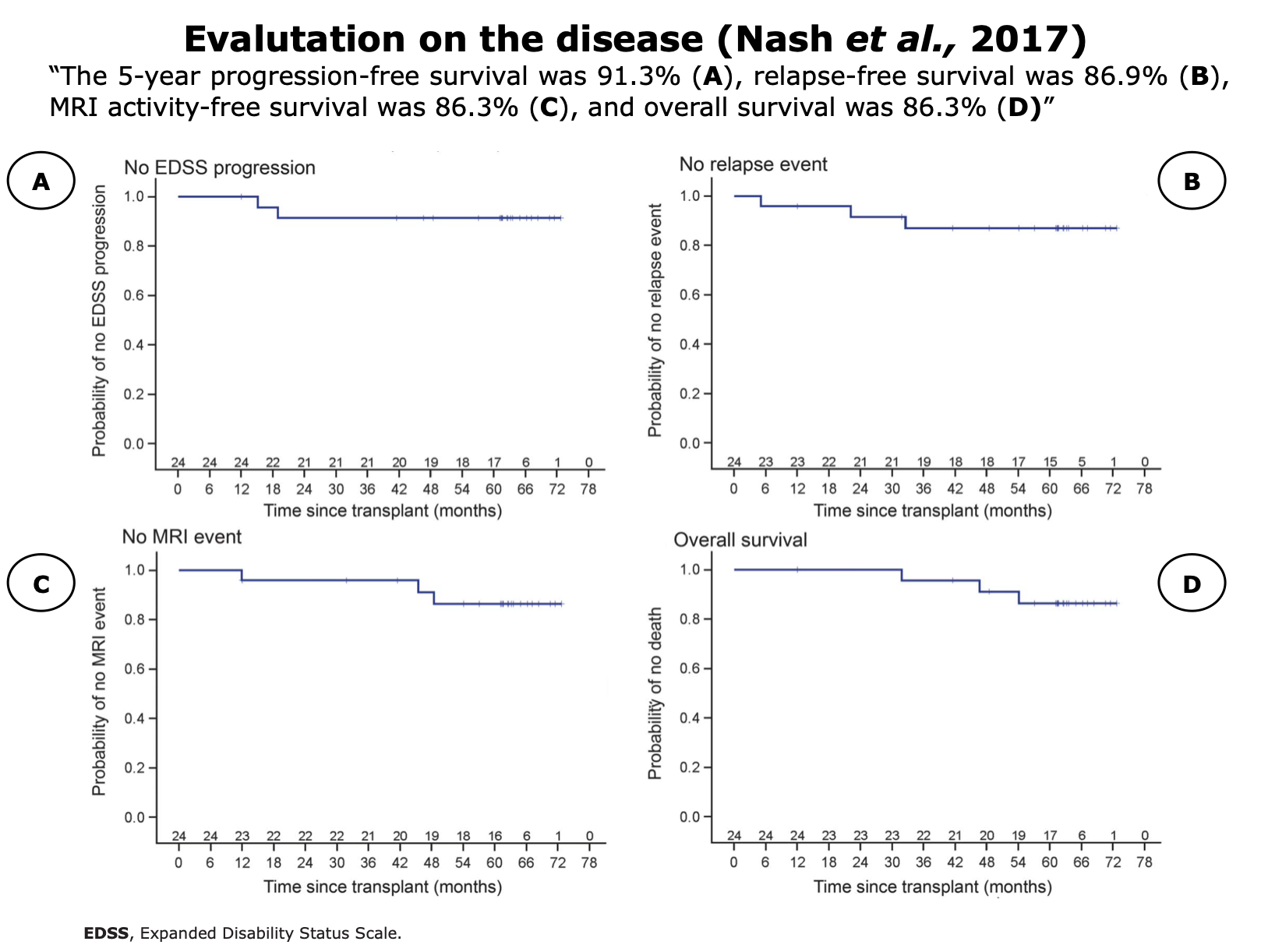
Figures from Nash et al. “High-dose immunosuppressive therapy and autologous HCT for relapsing-remitting MS”. Neurology (2017)
Limitation of this study: “A limitation of this study is that for secondary outcomes no corrections have been made for multiple comparisons, as this pilot study was hypothesis-generating and not a formal test of specific hypotheses.”
In this study, 41 pwMS underwent transplant at five Brazilian centers. A total of 21 patients were included in group 1 (BEAM) underwent AHSCT (or transplant) between 2001 and 2004, while 20 patients in group 2 (CY) underwent transplant between 2004 and 2006, allowing for a comparative analysis between both groups. 80.4% of these 41 patients had SPMS and the mean age was 42 years.
The objectives of this study were “to compare them [41 patients] by evaluating the clinical response to treatment using EDSS and with MRI before and after HSCT; complication and mortality rates after HSCT; and QoL before and after HSCT.”
None of the participants experienced adverse reactions, such as high blood pressure, fever, or allergic responses, during the graft infusion. There was no statistically significant difference between the two groups concerning the incidence of febrile neutropenia and pneumonia.
During the post-AHSCT period, 48% of patients experienced complications, most commonly urinary tract infections, affecting 7 individuals (18.4%). Although group 1 (BEAM) had a higher proportion of complications after transplant, this difference was not statistically significant. When comparing the two conditioning regimens, the BEAM/ATG group had a higher complication rate during transplantation at 71.4%, compared to 40% in the CY/rATG group (P = 0.04).
In this study “the CY/rATG regimen seems to be associated with similar outcome results, but presented less toxicity when compared with the BEAM/hATG regimen.
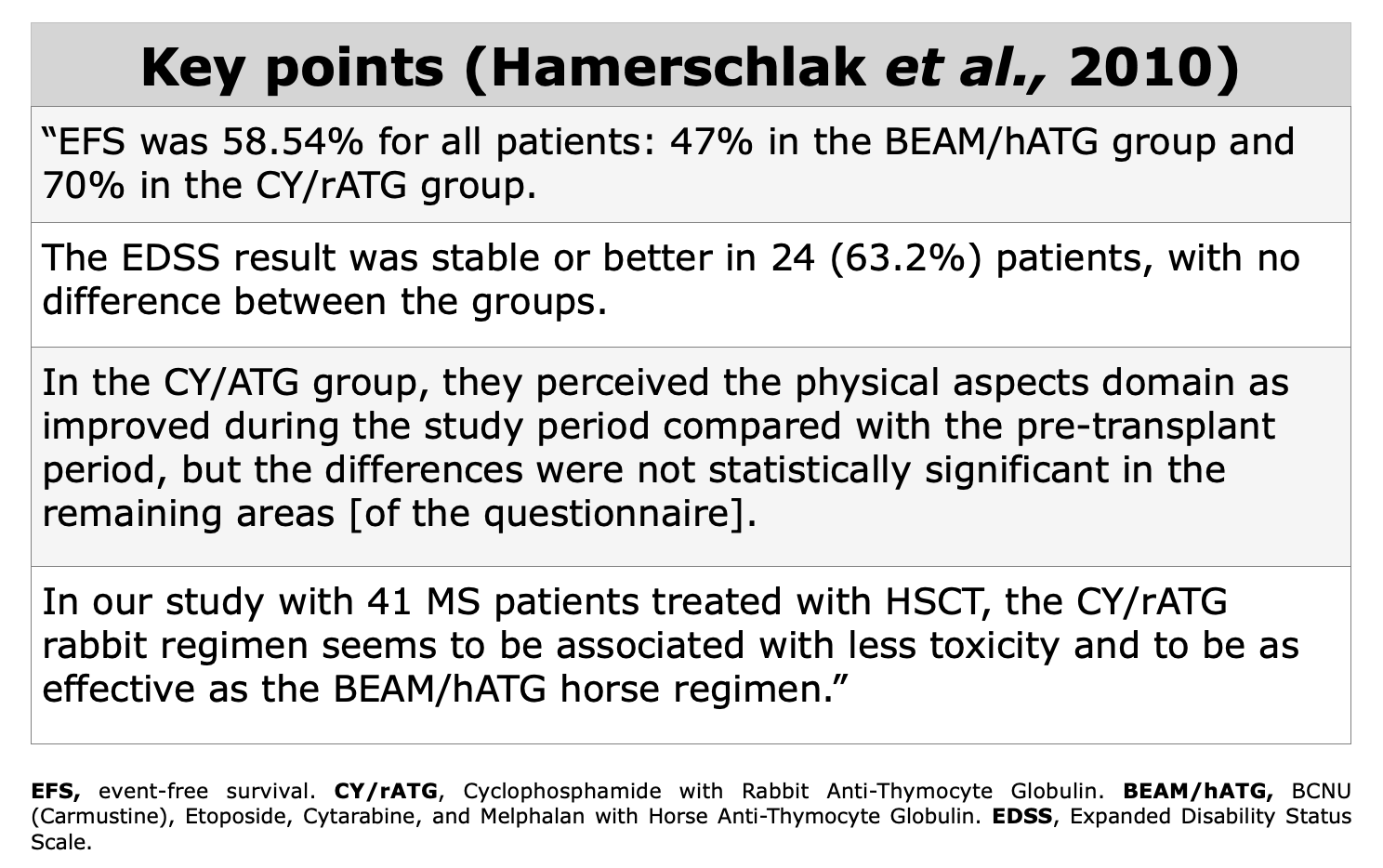
Long-term follow- up would be required to fully assess the differences in therapeutic effectiveness between the two regimens.” (Hamerschlak et al., 2010).
Limitations: “the use of two different sources of ATG, the involvement of various transplant centers, the analysis of two different conditioning regimens used in different time periods, and the relatively short period of follow-up.” (Hamerschlak et al., 2010).
Observational Retrospective Studies
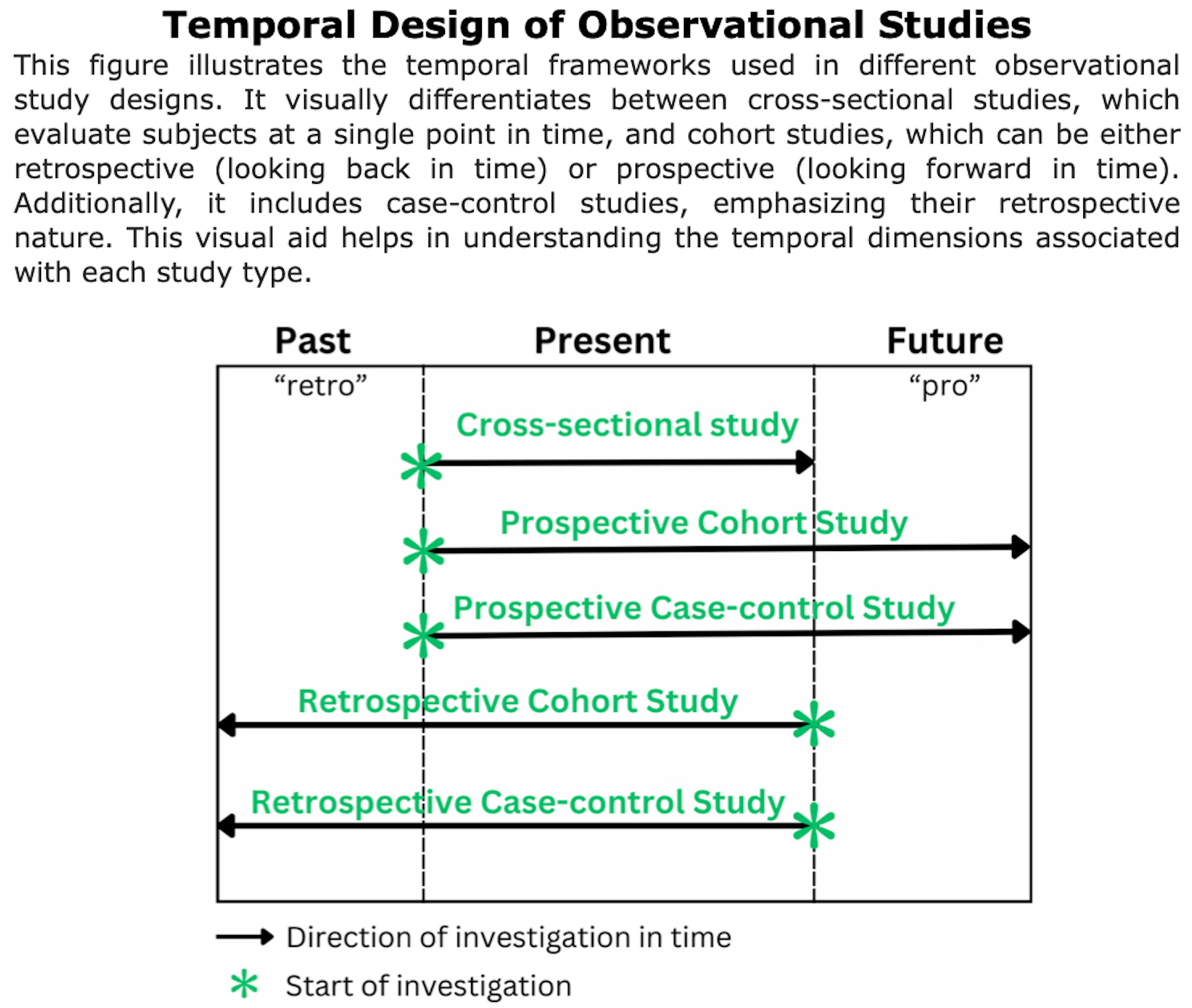
Definition of retrospective studies: “Retrospective cohort studies, also known as historical cohort studies, are carried out at the present time and look to the past to examine medical events or outcomes. In other words, a cohort of subjects selected based on exposure status is chosen at the present time, and outcome data (i.e. disease status, event status), which was measured in the past, are reconstructed for analysis.” (Song et al., 2010).
These studies are “observational” because the researchers do not intervene or alter the course of events; instead, they analyze past data to find correlations or outcomes.
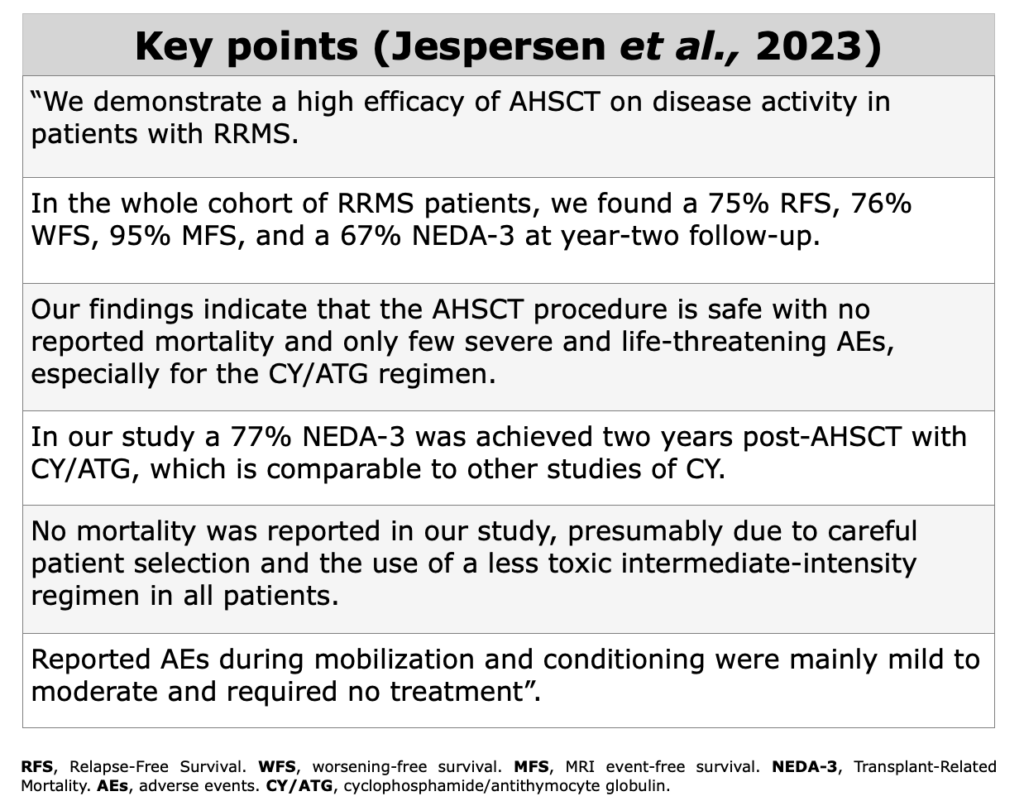
Jespersen et al., 2023 “Autologous hematopoietic stem cell transplantation of patients with aggressive relapsing-remitting multiple sclerosis: Danish nation-wide experience”. MSARD
“The purpose of this study is to describe the Danish experience with AHSCT focusing on patient characteristics, potential complications, and efficacy.” (Jespersen et al., 2023).
In this retrospective observational study were investigated 32 pwMS with RRMS treated with AHSCT from May 2011 to May 2021 in a single-center in Denmark: 7 patients underwent BEAM while 25 CY (cyclophosphamide).
No treatment related mortality and only few severe AEs (adverse events) were observed. In this study the authors found “75% RFS, 76% WFS, 95% MFS, and a 67% NEDA-3 at year-two follow-up.”
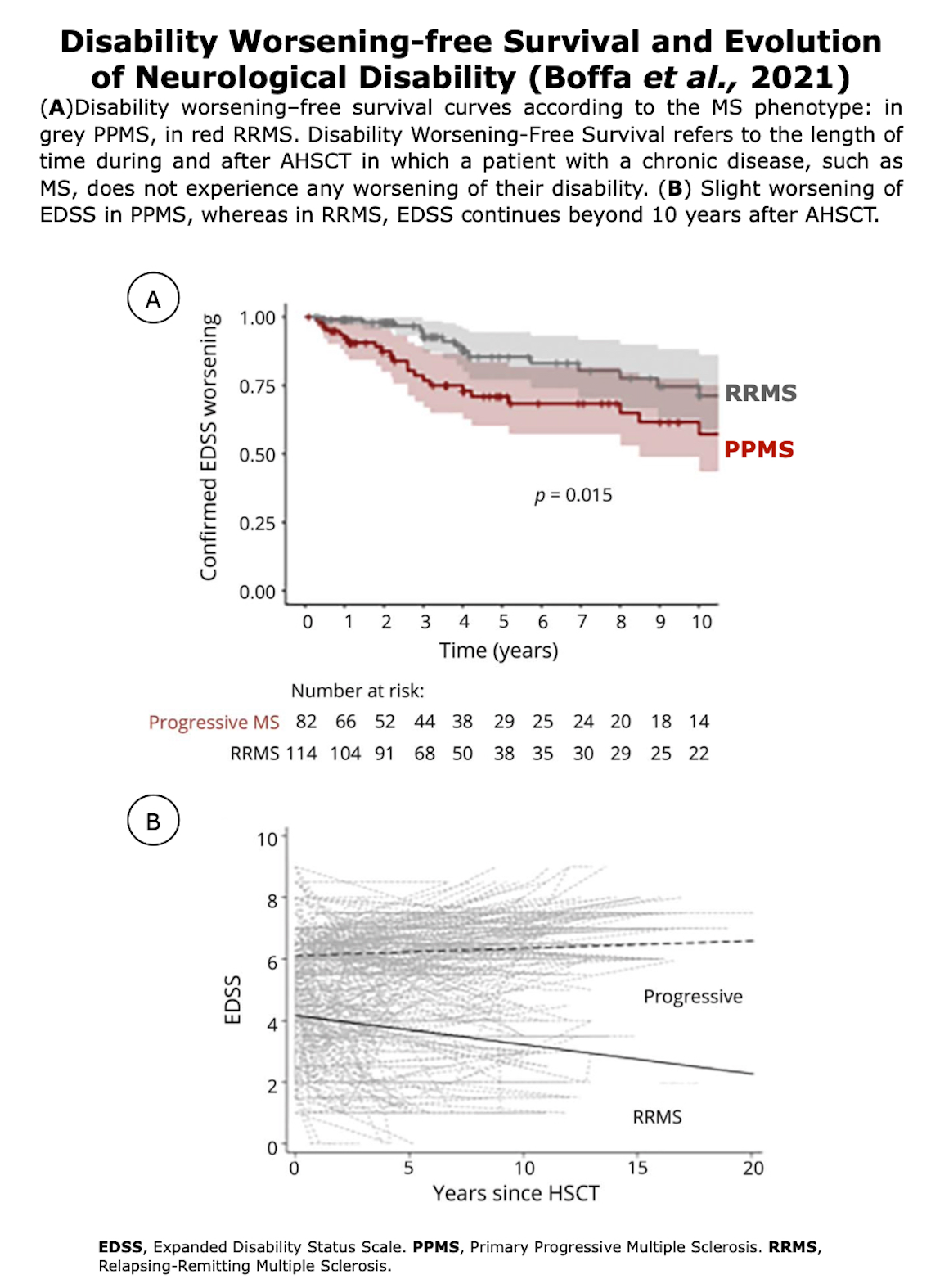
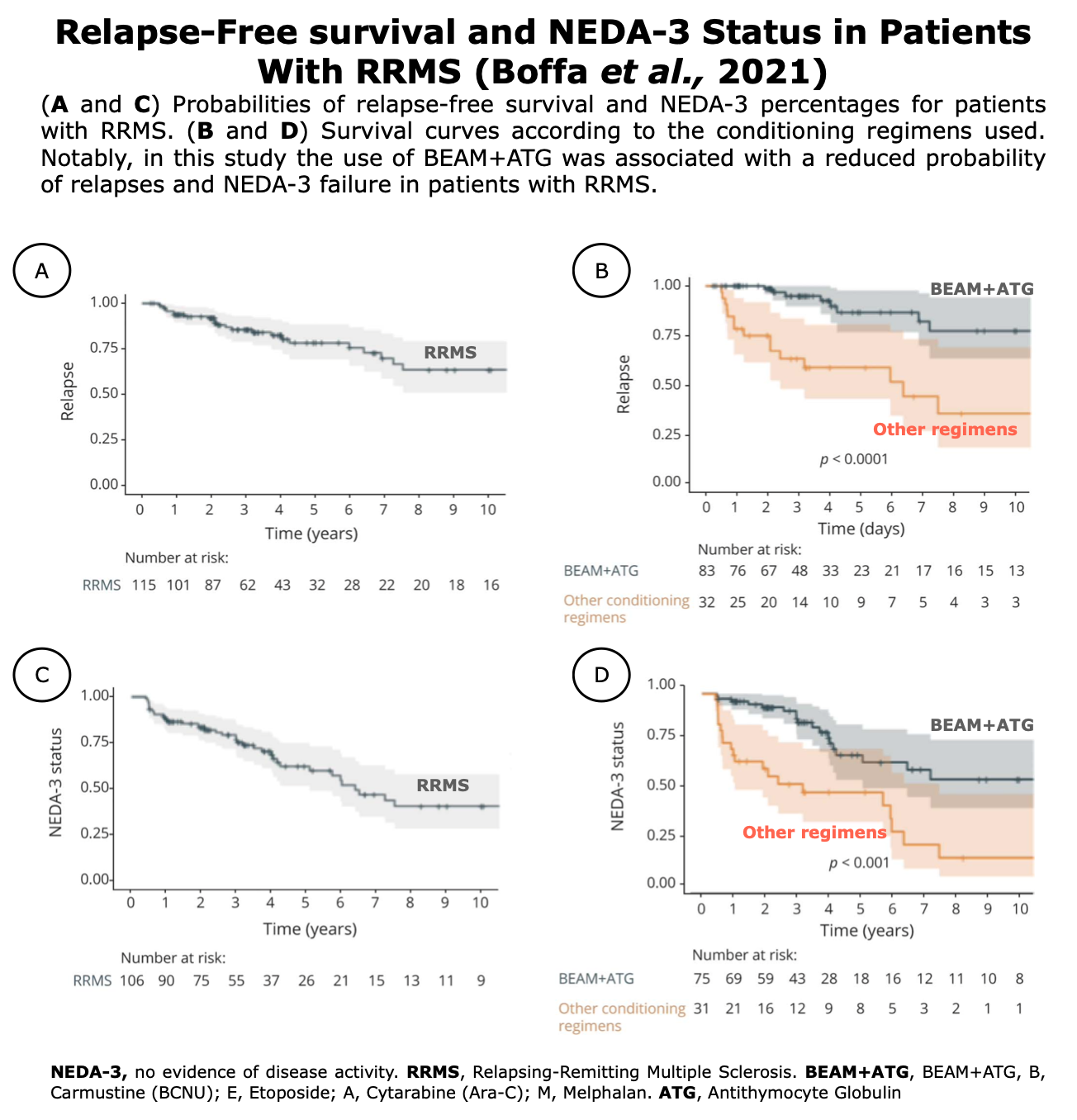
Boffa et al., 2021 “Long-term Clinical Outcomes of Hematopoietic Stem Cell Transplantation in Multiple Sclerosis”. Neurology
Boffa et al., 2021 published a multicentre cohort study, the team collected data from 210 patients who underwent AHSCT between 1997 and 2019 in 20 Italian MS centers. At the time of AHSCT, 122 were classified as RRMS, 86 SPMS and 2 PPMS. The EDSS score median was 6.0 at the baseline. The study compared different types of conditioning protocols.
The main objective was “To determine whether AHSCT is able to induce durable disease remission in people with MS” Boffa et al., 2021.
According to the authors this study generated Class IV evidence of long-term effects of AHSCT in people with aggressive MS, due to the analyses of the primary end-points (long-term 6-month confirmed disability worsening as measured by EDSS) and secondary end-points: EDSS post-ASHCT, relapses, MRI inflammatory activity, the proportion of patients achieving NEDA status; the effect of the different conditioning regimens on long-term outcomes; and the early TRM.
“AHSCT prevents disability worsening in the majority of patients and induces durable improvement in disability in patients with RRMS. The BEAM + ATG conditioning protocol is associated with a more pronounced suppression of clinical relapses and MRI inflammatory activity” (Boffa et al., 2021).

Figures from Boffa et al. “Long-term Clinical Outcomes of Hematopoietic Stem Cell Transplantation in Multiple Sclerosis”. Neurology (2021)
Figures from Boffa et al. “Long-term Clinical Outcomes of Hematopoietic Stem Cell Transplantation in Multiple Sclerosis”. Neurology (2021)
Limitations of this study: “First, the EDSS score raters were not blinded to treatment, and this could have introduced some bias. However, the long-term design of this study has partially mitigated this measurement bias. Second, we had no information about the time between last clinical relapse and start of transplantation AHSCT, and we could not correct for this confounder when analyzing EDSS score improvement over time, which thus can be overestimated. Third, clinical and MRI assessments were not systematically performed throughout the study. To overcome this bias, only patients with 6-month confirmed EDSS score assessment and yearly MRI records were included in the analysis of treatment effects.” (Boffa et al., 2021).
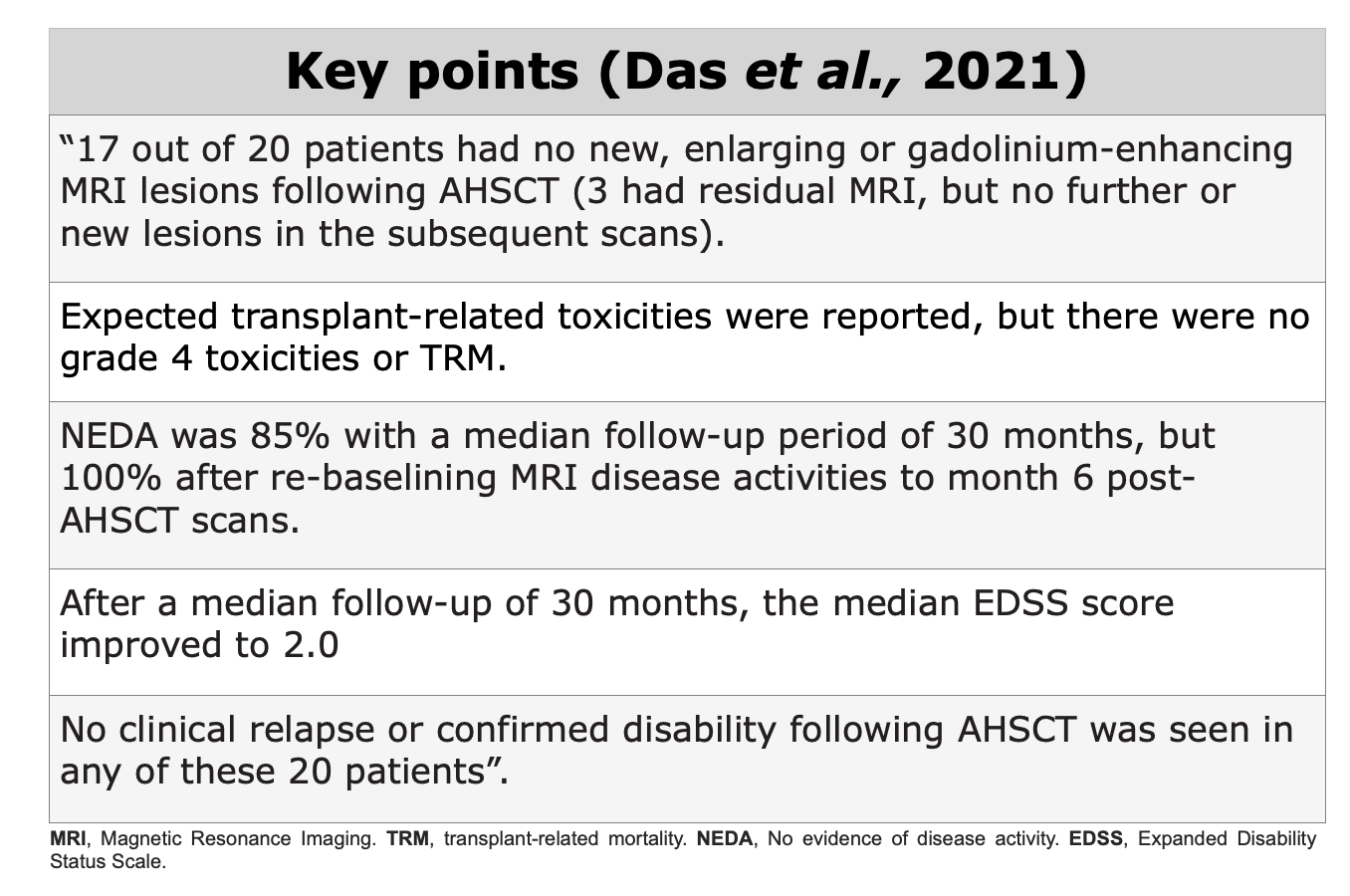
Das et al., 2021. “Autologous haematopoietic stem cell transplantation as a first-line disease-modifying therapy in patients with “aggressive” multiple sclerosis”. Multiple Sclerosis Journal.
This observational and muticentre study evaluated efficacy and safety of AHSCT as a first-line treatment in patients with “aggressive” MS, who underwent AHSCT as a first-line DMT in Sheffield (United Kingdom), Uppsala (Sweden), Ottawa (Canada), Chicago (United States) and Florence (Italy), with a median age of 28.
None of the 20 patients received any other DMT prior to transplant. The median follow-up among the group was 30 months. At the time of publication, this study included the largest cohort of pwMS with “aggressive” MS who received AHSCT as a first-line treatment.
“The treatment was safe and highly effective in inducing rapid and sustained disease remission with a significant improvement of disability” (Das et al., 2021).
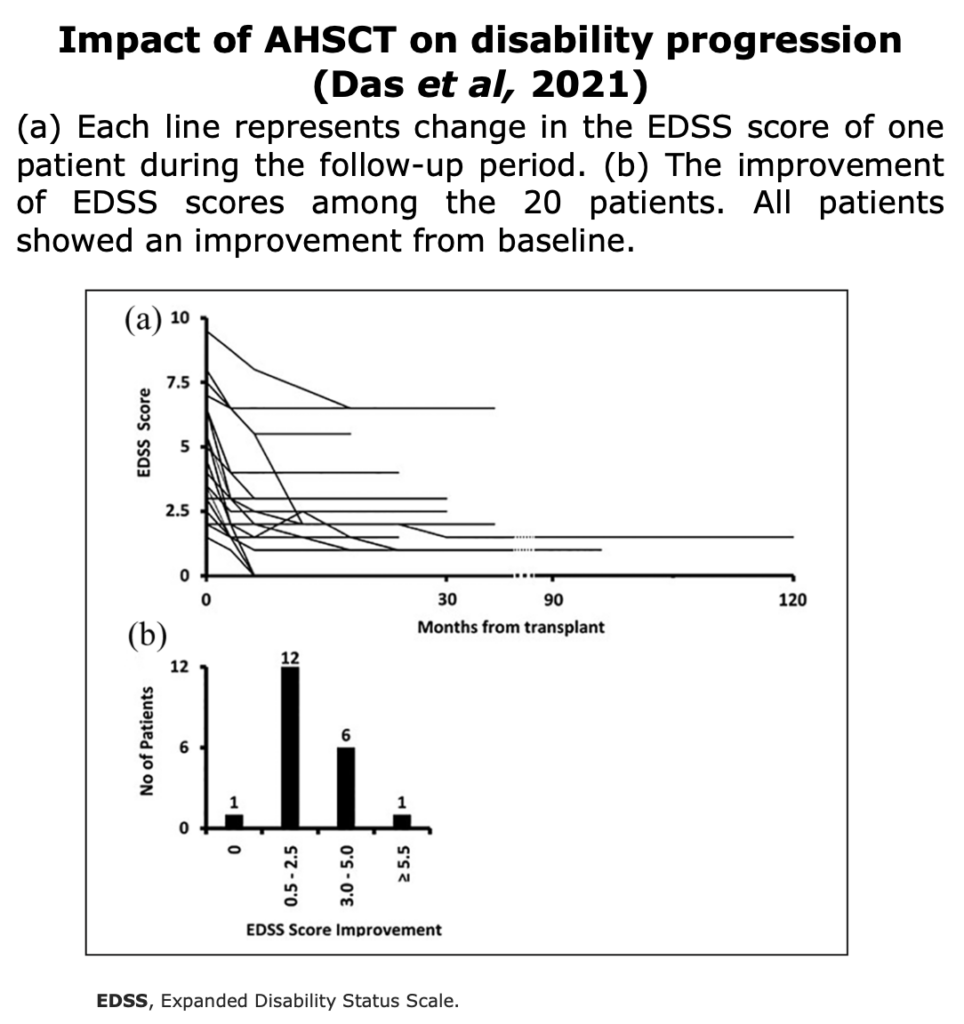
Figures from Das et al. “Autologous haematopoietic stem cell transplantation as a first-line disease- modifying therapy in patients with “aggressive” multiple sclerosis”. Multiple Sclerosis Journal (2021)
Limitations of this study: The main limitation of this study was the small cohort. Three different regimens were used: Bu-Cy-ATG (4 patients), BEAM- ATG (4 patients) and Cy-ATG (12 patients). This is the main reason why, in this study, the team decided not to compare transplant with other standard DMTs.
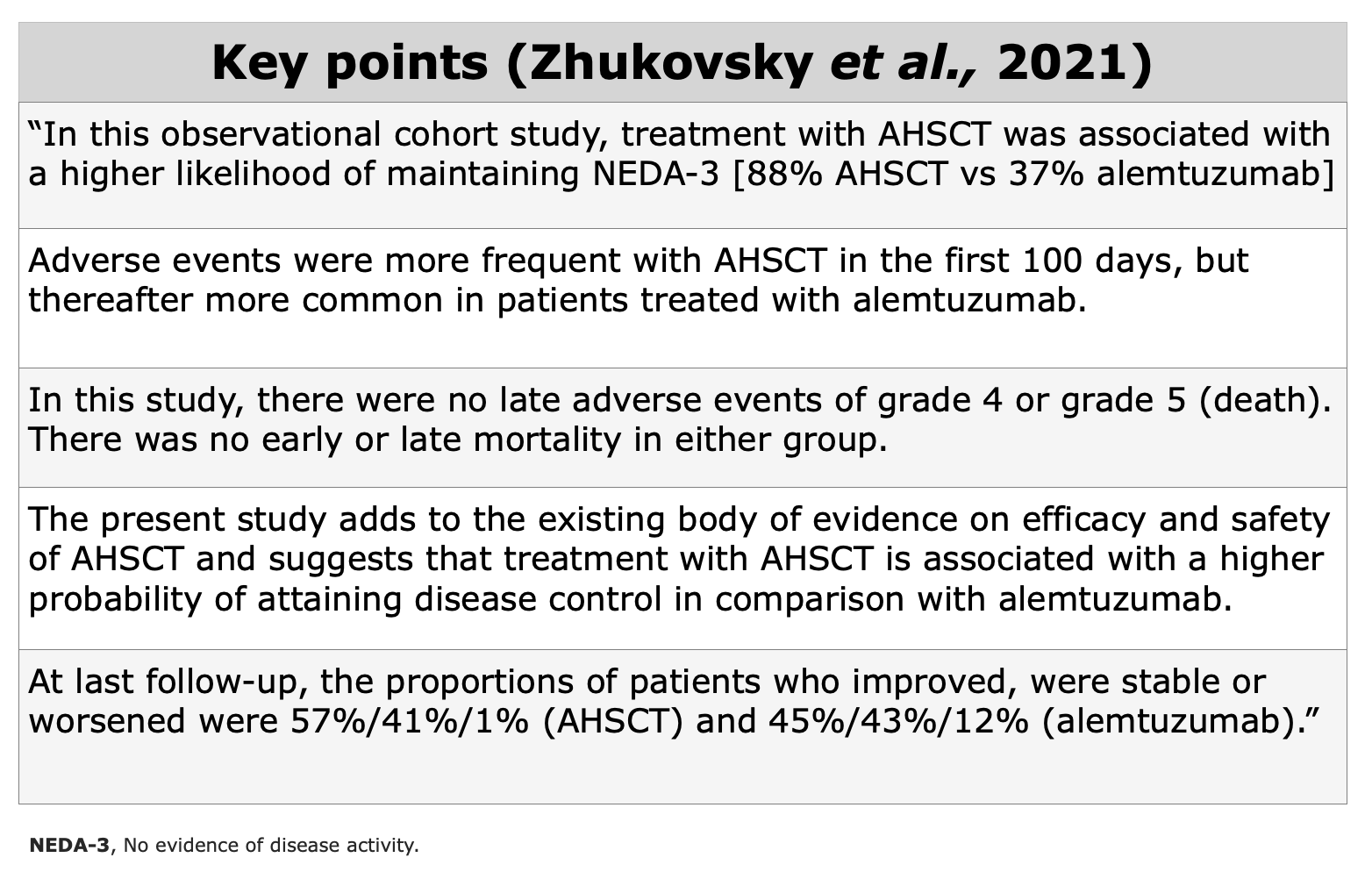
Zhukovsky et al., 2021. “Autologous haematopoietic stem cell transplantation compared with alemtuzumab for relapsing–remitting multiple sclerosis: an observational study”. Journal of Neurology, Neurosurgery & Psychiatry.
The main objective of this study was “to compare outcomes after treatment with AHSCT and alemtuzumab (ALZ) in patients with RRMS”. Zhukovsky et al., 2021.
In this observational study, Zhukovsky et al., compared the outcome and safety of patients with RRMS treated with AHSCT using a cyclophosphamide-based conditioning regimen (n=69) or alemtuzumab (n=75), at Uppsala University Hospital or Sahlgrenska University Hospital (Sweden) from 1 January 2011 to 31 December 2018.
“All alemtuzumab treated patients received at least one dose, 72 received two doses and 17 received three or more doses of alemtuzumab”. Zhukovsky et al., 2021.
“The primary endpoint was the Kaplan-Meier estimate of NEDA-3 at 3 years from the day of haematopoietic stem cell infusion or the day of the first infusion of alemtuzumab” Zhukovsky et al., 2021. While secondary endpoints were the absence of MRI events, clinical relapses, freedom from Confirmed Disability Worsening (CDW), the ARR after treatment, proportion of patients (EDSS ≥2) with CDI/stability/CDW, the EDSS change between baseline and follow-up at one, two and 3 years, and adverse events of grade 3 or higher.
“The use of different conditioning regimens and differences in DMD treatment prior to AHSCT could affect the occurrence of secondary autoimmunity and methodological differences in identifying and classifying adverse events could also contribute to the discrepancies between different studies” Zhukovsky et al., 2021.
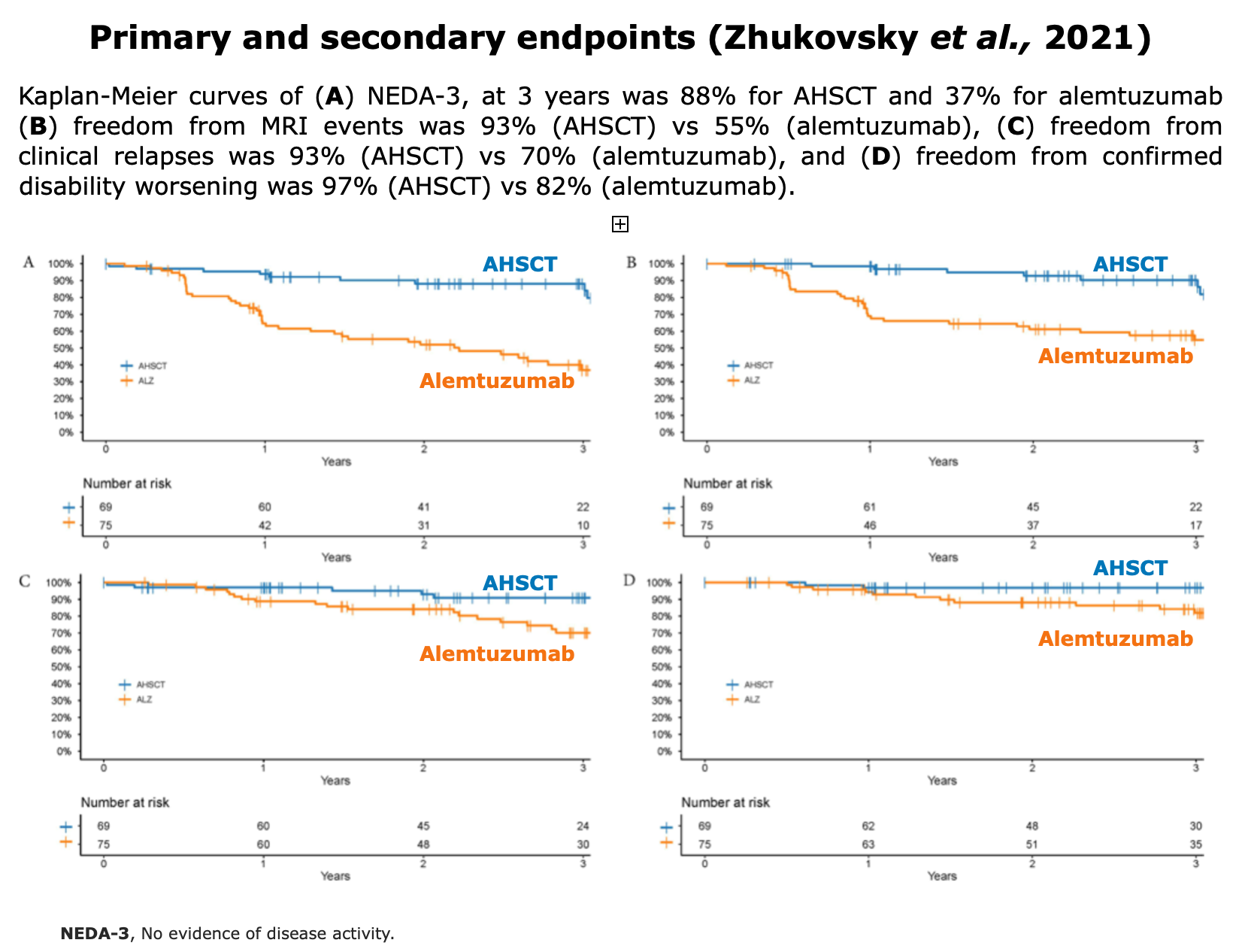
Figures fromZhukovsky et al. “Autologous haematopoietic stem cell transplantation compared with alemtuzumab for relapsing–remitting multiple sclerosis: an observational study”. J Neurol Neurosurg Psychiatry (2021)
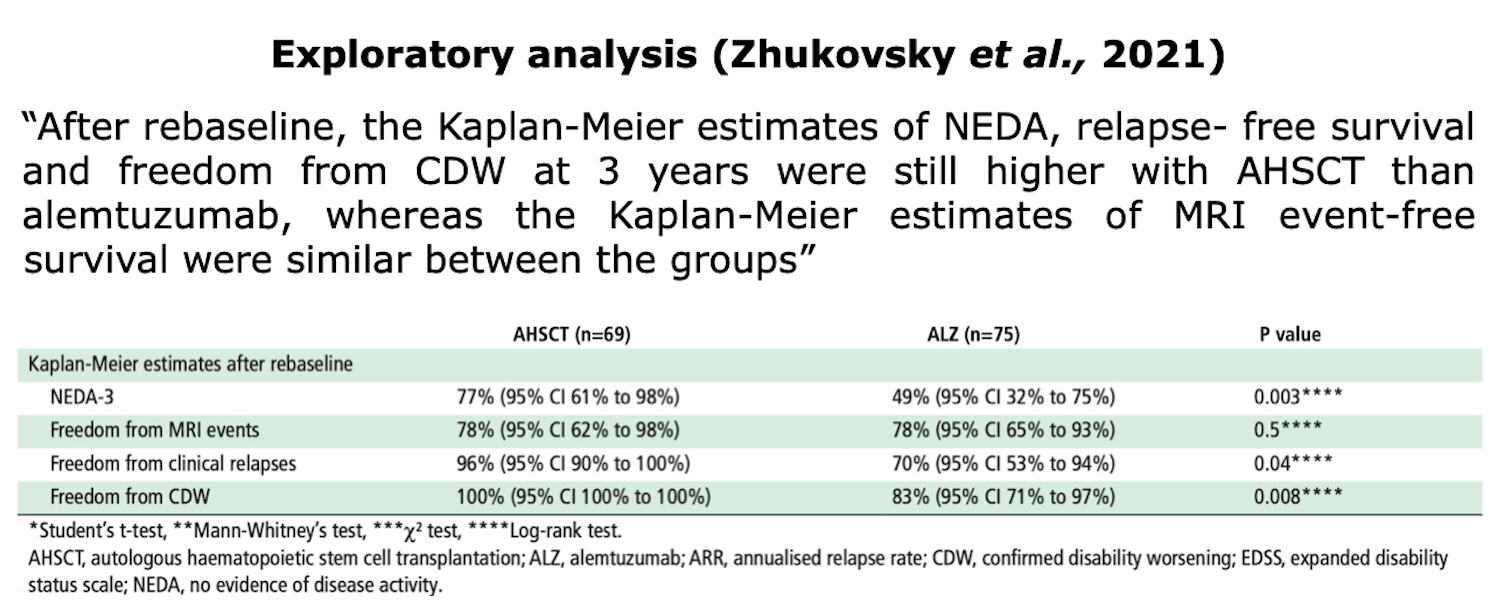
Table from Zhukovsky et al. “Autologous haematopoietic stem cell transplantation compared with alemtuzumab for relapsing–remitting multiple sclerosis: an observational study”. J Neurol Neurosurg Psychiatry (2021)
Limitation this study: “The main limitation of this study is the non-randomised intervention.” Zhukovsky et al., 2021.
Nicholas et al., 2021 “Autologous Hematopoietic Stem Cell Transplantation in Active Multiple Sclerosis. A Real-world Case Series”. Neurology
The cohort in this study includes 120 pwMS (52% had progressive MS, primary or secondary, and 48% had RRMS), treated with AHSCT at 2 centers in London, between 2012 and 2019 with at least 6 months of follow-up or died at any time. The mean follow-up for the entire cohort was 21 months. 70 (58%) out of 120 patients have tried high-efficacy DMTs before AHSCT.

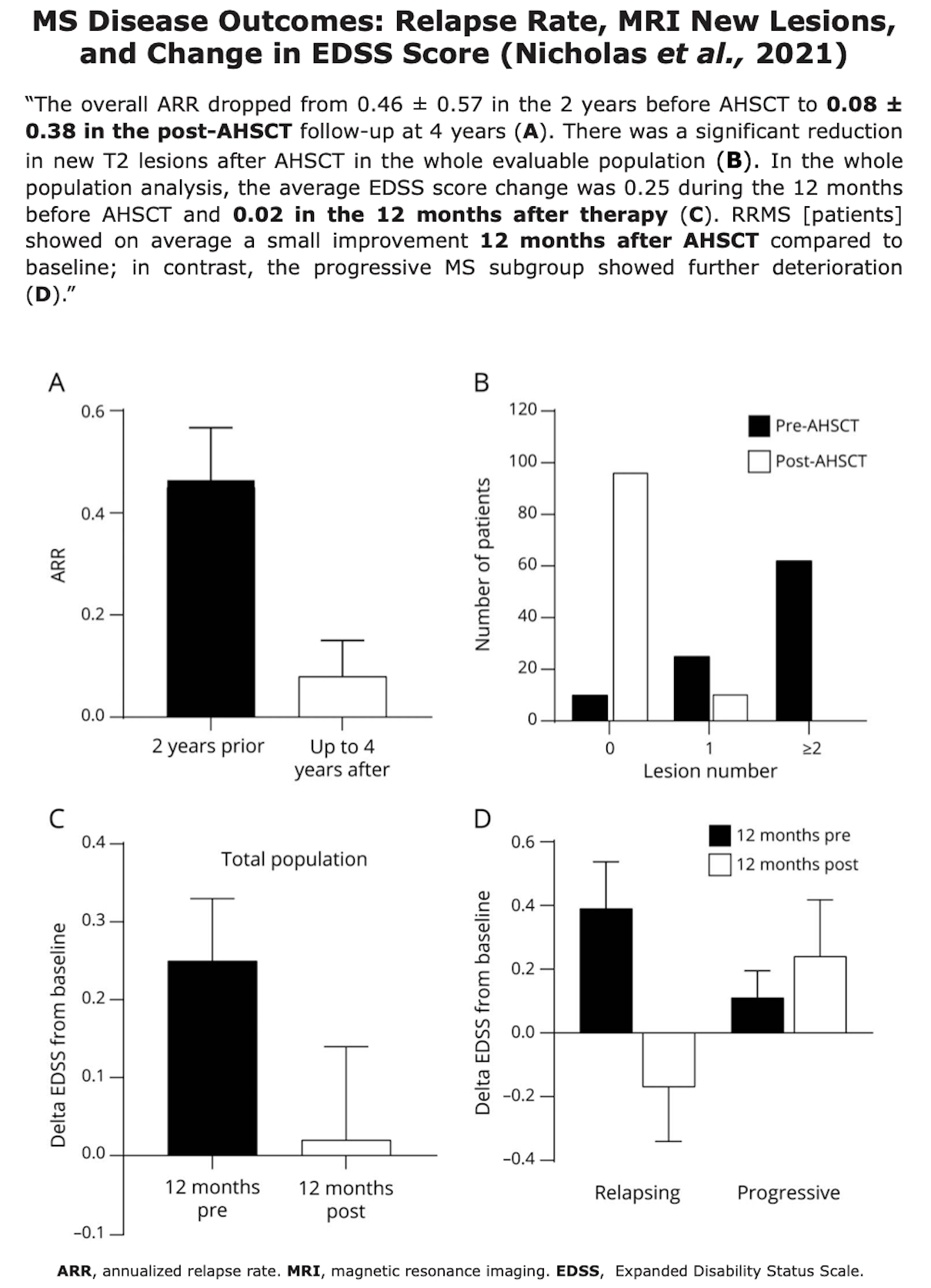

This study, a Class IV evidence due to its uncontrolled, open-label design, states that the “efficacy outcomes of AHSCT in this real-world cohort are similar to those reported in more stringently selected clinical trial populations, although the risks may be higher.” Nicholas et al., 2021
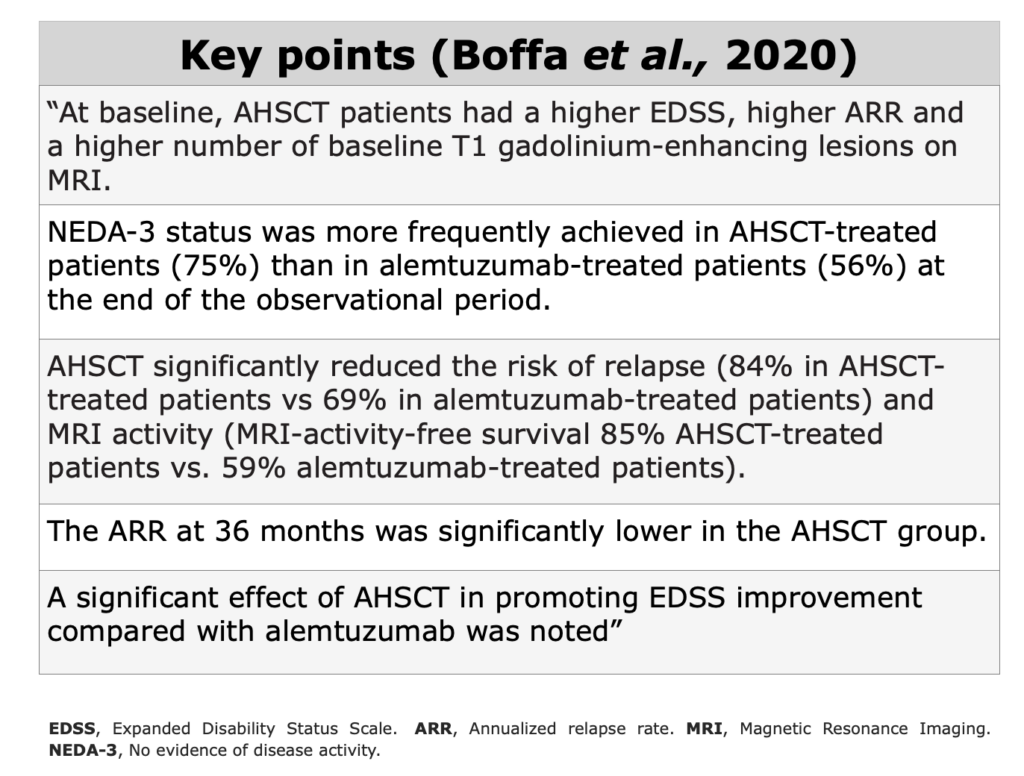
Boffa et al., 2020 “Aggressive multiple sclerosis: a single-centre, real-world treatment experience with autologous haematopoietic stem cell transplantation and alemtuzumab”. European Journal of Neurology
The aim of this single-centre and retrospective study was comparing transplant (or AHSCT) vs alemtuzumab in aggressive RRMS. The cohort consisted of 25 AHSCT- and 32 alemtuzumab-treated RRMS patients.
“Alemtuzumab and AHSCT are effective treatment choices for aggressive MS. AHSCT seems to be superior to alemtuzumab in inducing complete disease control and in promoting short-term disability improvement.” Boffa et al., 2020.

Figures from Boffa et al. “Aggressive multiple sclerosis: a single-centre, real-world treatment experience with autologous haematopoietic stem cell transplantation and alemtuzumab”. European Journal of Neurology (2020)
Limitation of this study: this was a retrospective and the two groups were significantly unbalanced in terms of age, EDSS score, ARR (annualized relapse rate), and MRI activity at the baseline evaluation.
Finally, the clinical assessment was not blinded, and this factor may introduce some bias.
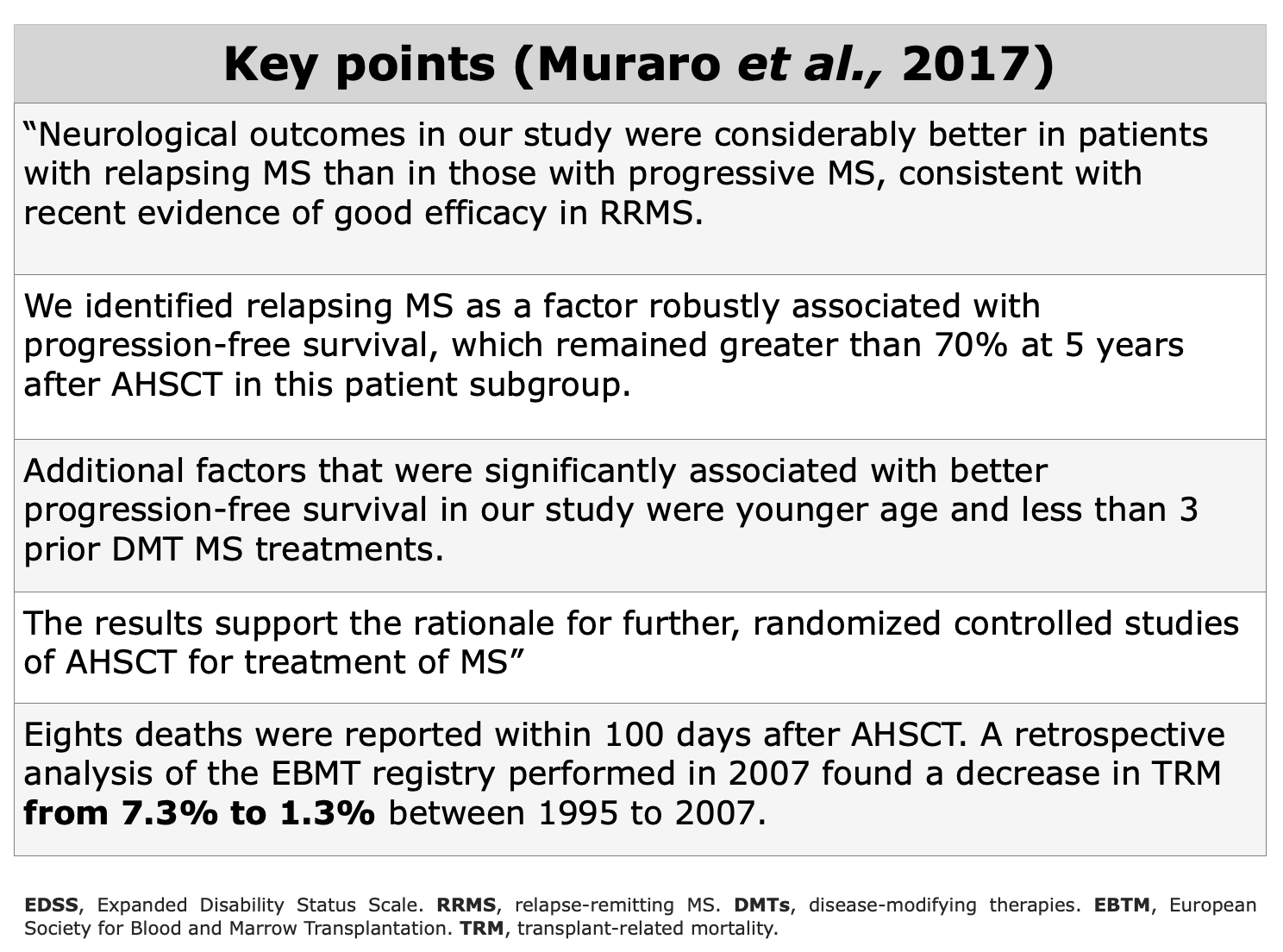
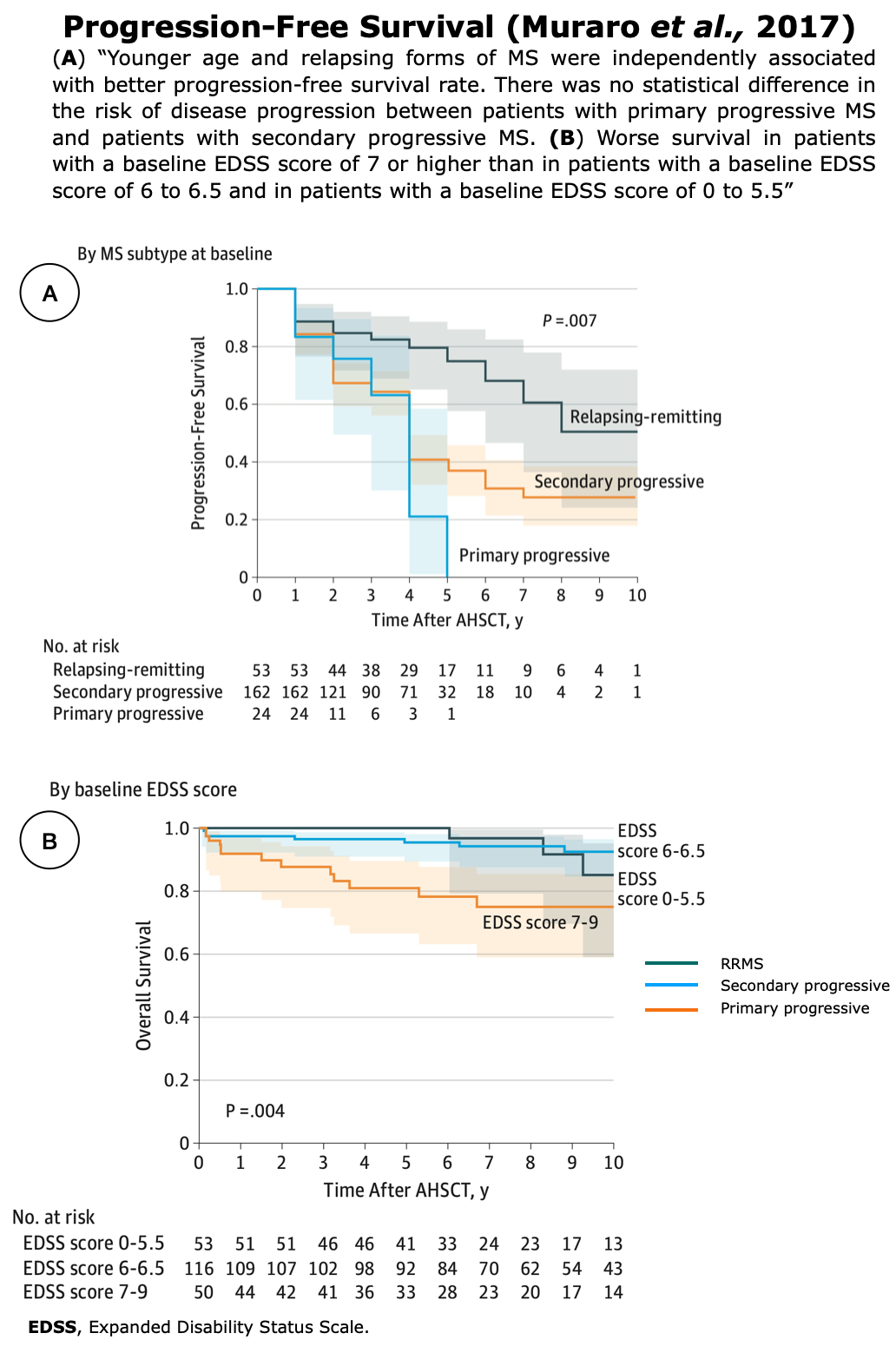
This multicenter, observational, retrospective cohort study, collected data from 25 centers, in 13 countries for 281 patients who underwent AHSCT from 1995 and 2006. This study was performed through collaboration between the Center for International Blood and Marrow Transplant Research (CIBMTR) Autoimmune Disease Working Committee and the EBMT Group Autoimmune Disease Working Party. CIBMTR contributed data for 111 patients, while the other 170 patients were taken from the EBMT registry. 46 patients were classified as RRMS, 17 were progressive relapsing, 32 were primary progressive and 186 were SPMS.
“At the time of AHSCT, 171 of 281 patients (60.9%) had received 2 or more prior MS treatments” and “the median EDSS score before mobilization of peripheral blood stem cells was 6.5 (range, 1.5-9), indicating moderately advanced disability on average” Muraro et al., 2017.
Different conditioning protocols were used and the proportions of patients who received high-, intermediate- or low-intensity conditioning regimens were similar in the CIBMTR cohort, whereas 151 of 170 patients (88.0%) received intermediate-intensity regimen.
As reported by the authors, the primary outcomes were MS progression-free survival and overall survival. Eight deaths (2.8%) were reported within 100 days after AHSCT.
This data may be controversial. However “a retrospective analysis of the EBMT registry performed in 2007 found a decrease in TRM (transplant-related mortality) from 7.3% in transplants for MS performed from 1995 to 2000 (inclusive) to 1.3% in transplants for MS performed from 2001 to 2007 (inclusive). In a 2010 update, the 100-day mortality in the entire registry was 2%, half of that in the 2005 report.” Muraro et al., 2017. The decrease observed over the years is likely due to better patient selection, which excludes those with advanced disabilities who are at higher risk of complications, and the less frequent use of intensive conditioning regimens among this population.
Figures from Muraro et al. “Long-term Outcomes After Autologous Hematopoietic Stem Cell Transplantation for Multiple Sclerosis”. JAMA Neurology (2017)
Limitation of this study: Muraro et al., 2017 reported that “The main limitation of our study is its partially retrospective nature. Although some of the data were obtained retrospectively from clinical records, we took many steps to optimize the analysis” and “our analysis included 57.0% (281 of 493) of the transplants registered with the
The median patient had tried two treatments before AHSCT (range 0–4). Previous treatments were: interferon β (n=36), natalizumab (n=21), glatiramer acetate (n=18), mitoxantrone (n=15), intravenous immunoglobulins (n=4), fingolimod (n=2) and rituximab (n=2). 4 patients had no previous treatment.
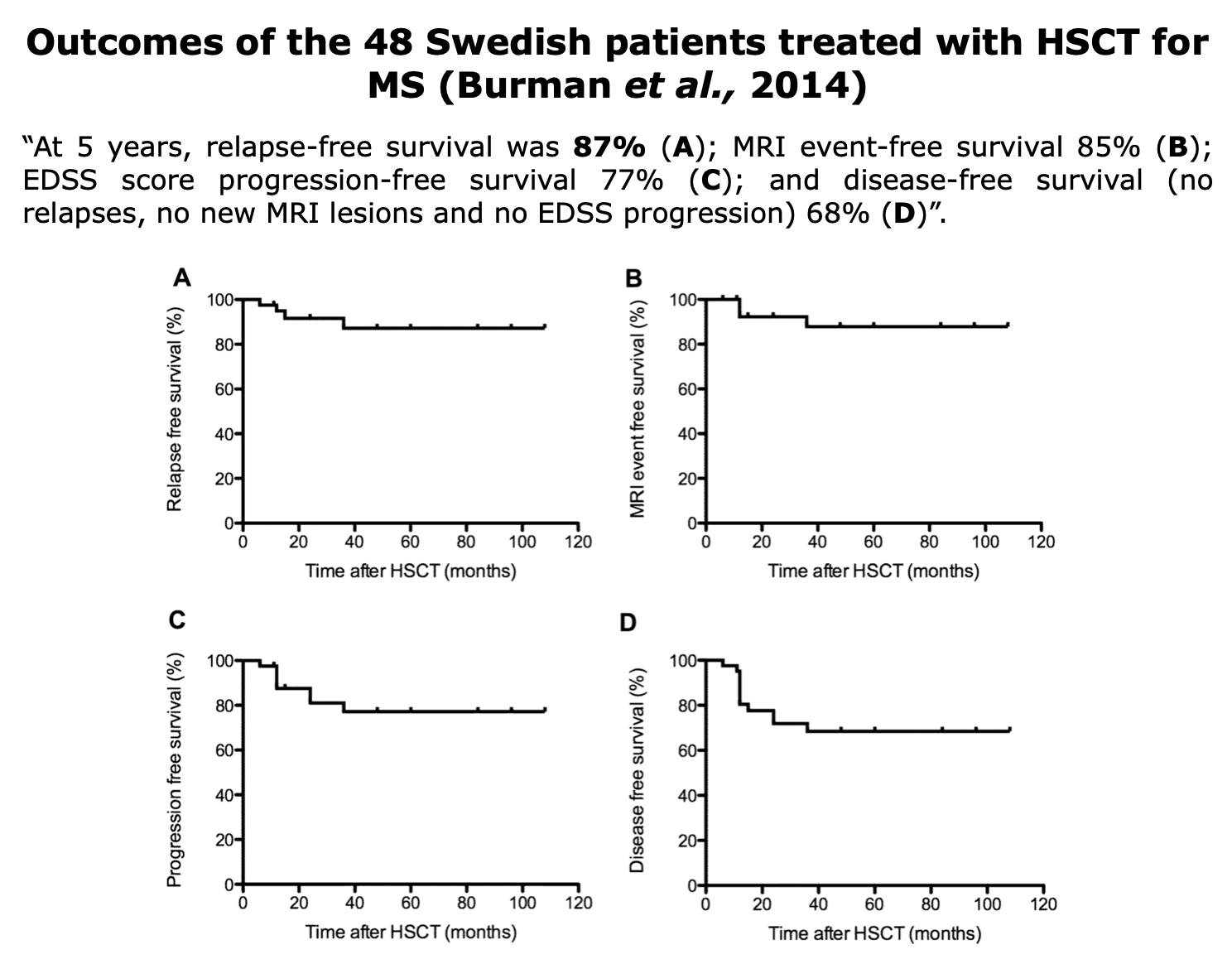
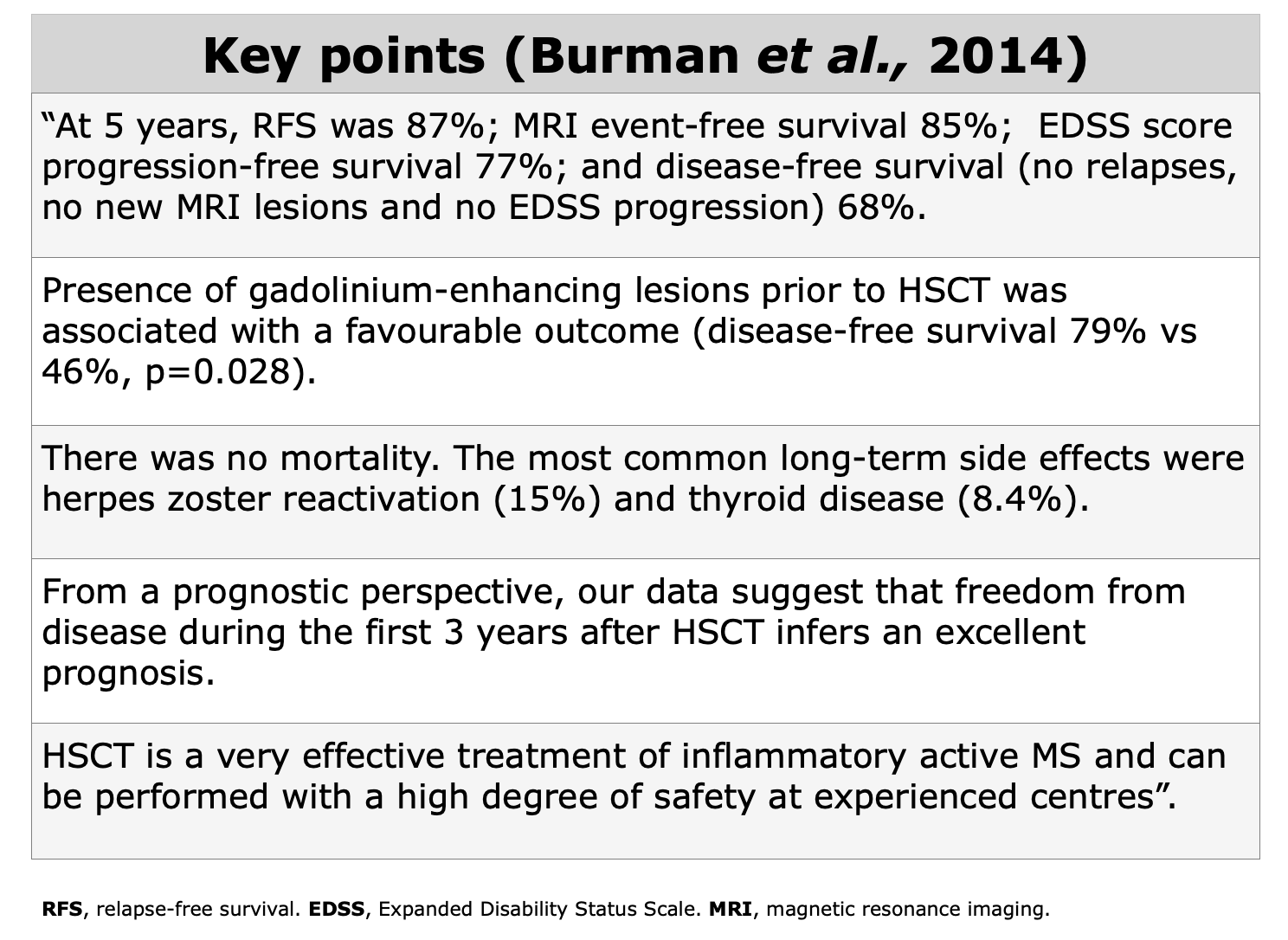
In this study “there was no mortality and no patient required treatment in the intensive care unit” Burman et al., 2014. There were reported expected side effects such as alopecia, anaemia, thrombocytopenia and leukopoenia, while late side effects consisted mainly of herpes zoster reactivation (8 patients) and thyroid disease (4 patients). Successful pregnancies were reported. No secondary malignacies were reported in this study.
Propensity Score Studies
Retrospective studies with propensity scores are observational studies that use statistical techniques to reduce bias and simulate some of the characteristics of RCTs.
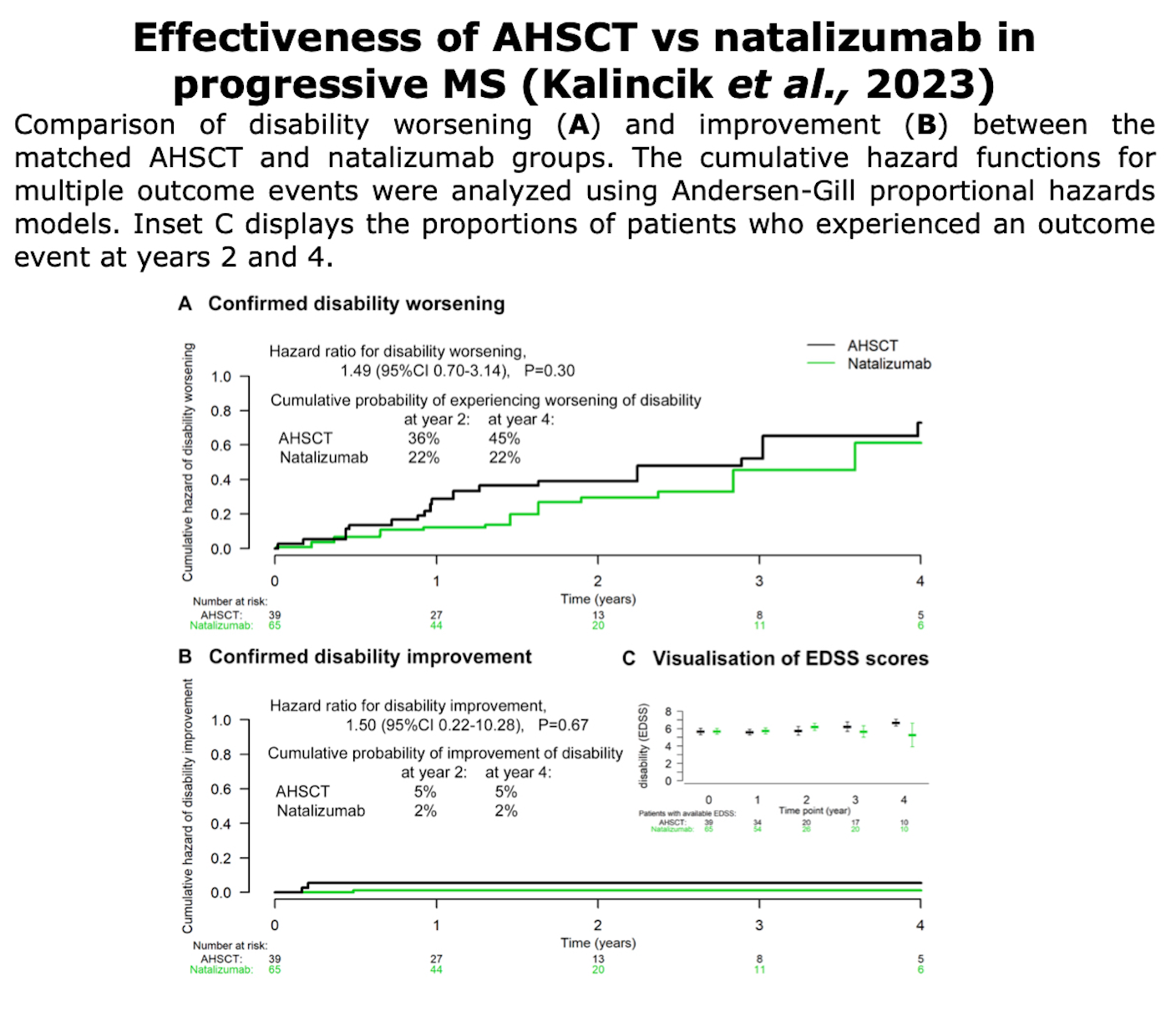
Kalincik et al., 2024. “Effectiveness of autologous haematopoietic stem cell transplantation versus natalizumab in progressive multiple sclerosis”. Journal of Neurology, Neurosurgery & Psychiatry.
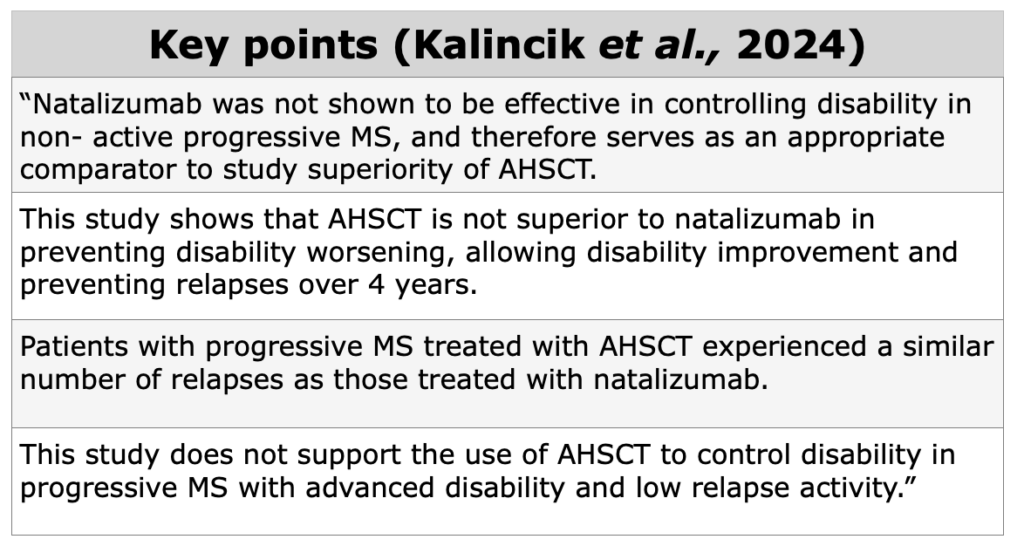
In this observational study, the authors used a composite cohort, comparing the effectiveness of AHSCT with natalizumab in progressive forms of MS (PPMS and SPMS). Kalincik et al., compared 39 eligible patients treated with AHSCT and 65 patients treated with natalizumab, using a composite cohort from 7 AHSCT MS specialized center and MSBase International Registry. Patients with relapses were excluded.
“The primary endpoint was the cumulative hazard of disability worsening. Secondary endpoints were the cumulative hazards of disability improvement, the on-treatment annualised relapse rate (ARR) and the cumulative hazard of relapses” Kalincik et al., 2024.
Figures from Kalincik et al. ”Effectiveness of autologous haematopoietic stem cell transplantation versus natalizumab in progressive multiple sclerosis“. J Neurol Neurosurg Psychiatry (2024)
According to the authors “AHSCT cannot be justified as a therapy among patients with progressive MS with low level of relapse activity” Kalincik et al., 2023. The study did not demonstrate differences between the two treatments.
Limitations of this study: 64.1% of the patients in each group, almost 2 out of 3 patients did not report whether and what types of treatment they had previously received.
The author included in this study pwMS who underwent different types of AHSCT (BEAM, busulfan with cyclophosphamide, and cyclophosphamide with anti-thymocyte globulin). However, it should be noted that BEAM has been shown to be more effective than cyclophosphamide (Boffa et al., 2021).

Figures from Kalincik et al. ”Effectiveness of autologous haematopoietic stem cell transplantation versus natalizumab in progressive multiple sclerosis”. J Neurol Neurosurg Psychiatry (2024)
Taken together, their results support the conclusion that the use of AHSCT to control disability in progressive MS patients with advanced disability and low relapse activity is not recommended.
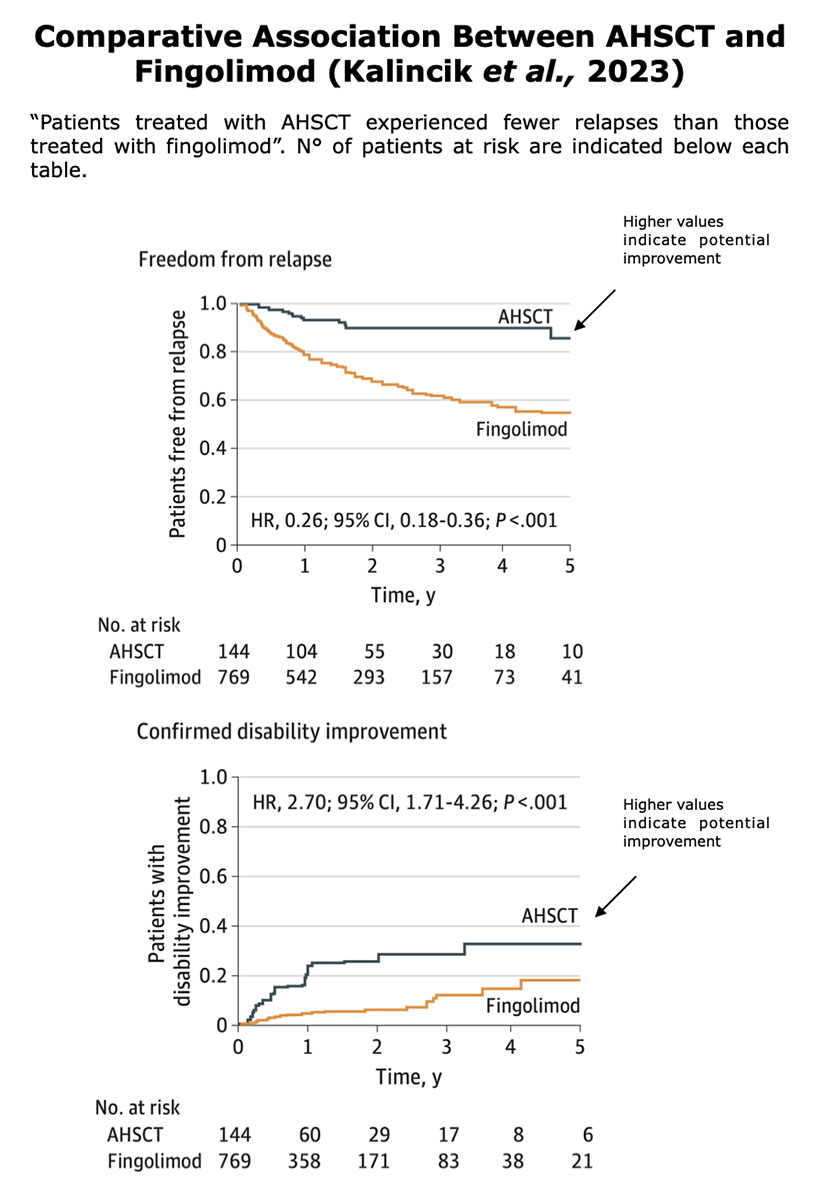
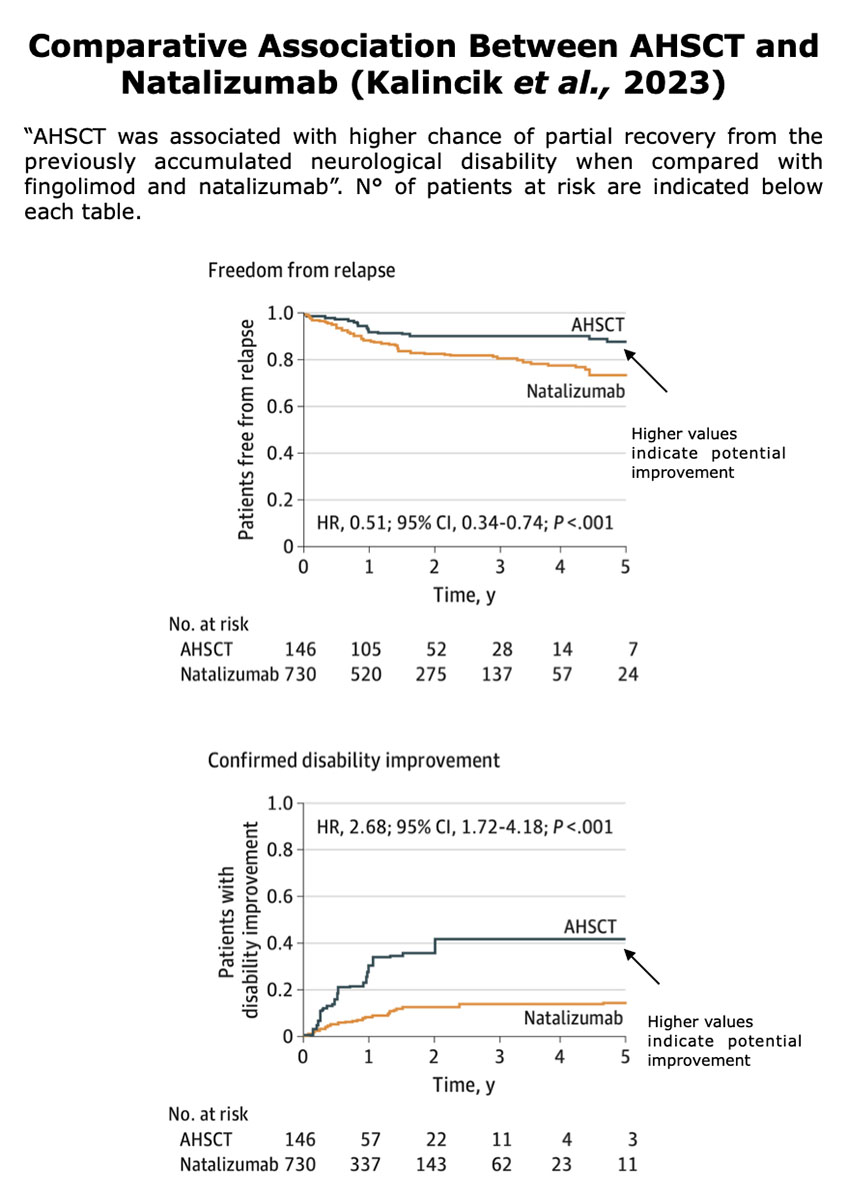
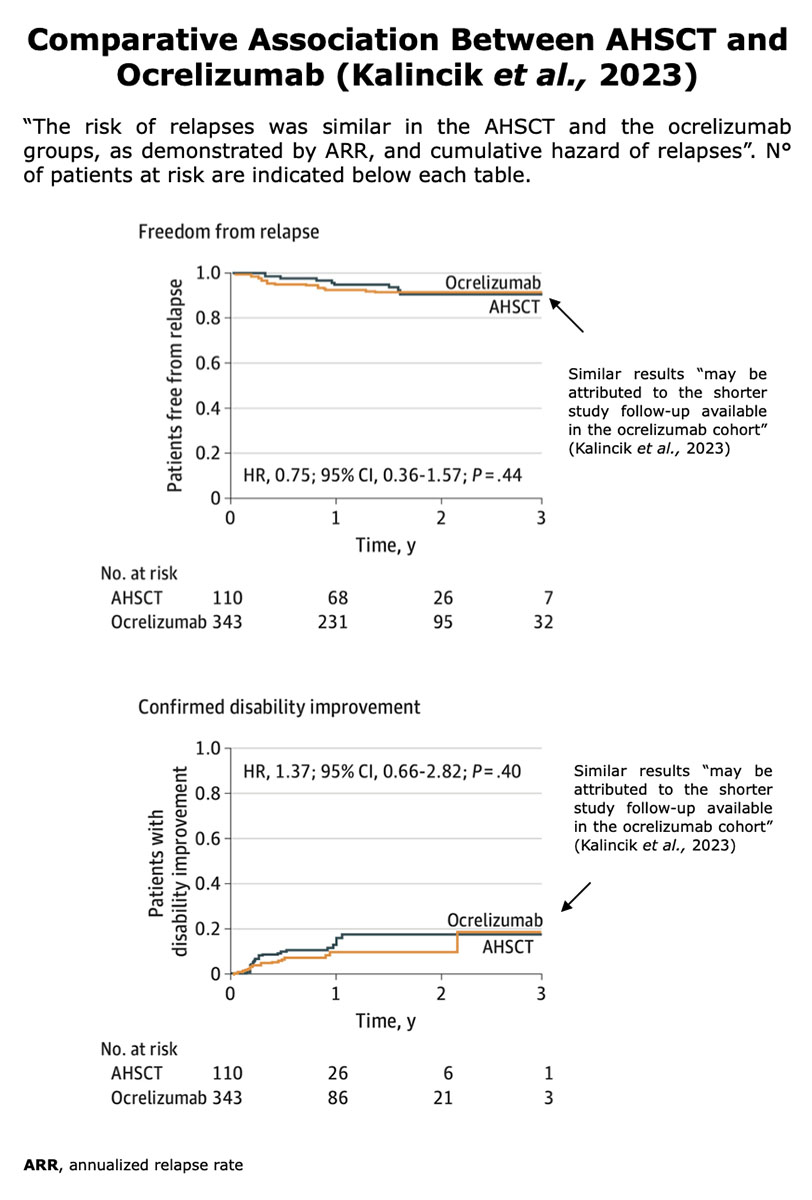
The objective of this study was “To compare the effectiveness of AHSCT vs fingolimod, natalizumab, and ocrelizumab in relapsing-remitting MS by emulating pairwise trials” Kalincik et al., 2023.
The data were collected from 6 specialist MS centers worldwide between May 2006 and December 2021 from 4915 individuals, of whom 167 were treated with transplant (3.4%), 2558 with fingolimod (52.0%), 1490 with natalizumab (30.3%) and 700 with ocrelizumab (14.2%). The study included patients with RRMS and had at least 2 years of follow-up with 2 or more disability assessments.
Patients were matched using a propensity score based on clinical and demographic characteristics. Both myelo-ablative and lympho-ablative, conditioning regimens were used among the AHSCT-treated patients.
Often, studies that draw data from MS registries lack certain information. The percentage of patients for whom it is unknown what type of DMTs were used before AHSCT is significantly higher than the percentage for whom data is available in the study.
Kalincik et al., 2023 considered as the main endpoint the annualized relapse rate (ARR) while on treatment with the study therapy, as per the standard analytical protocol while secondary end points were the “cumulative hazards of first postbaseline relapse and the proportions of patients free from disability worsening and with disability improvement”.
According to the authors “The results support AHSCT as highly efficacious when used to treat highly active relapsing-remitting MS. The association of AHSCT with preventing relapses is substantially superior to fingolimod, marginally superior to natalizumab, and, with a shorter follow-up, appears similar to ocrelizumab” (Kalincik et al., 2023).
Figures from Kalincik et al. “Comparative Effectiveness of Autologous Hematopoietic Stem Cell Transplant vs Fingolimod, Natalizumab, and Ocrelizumab in Highly Active Relapsing-Remitting Multiple Sclerosis”. JAMA Neurology (2023)
Figures from Kalincik et al. “Comparative Effectiveness of Autologous Hematopoietic Stem Cell Transplant vs Fingolimod, Natalizumab, and Ocrelizumab in Highly Active Relapsing-Remitting Multiple Sclerosis”. JAMA Neurology (2023)
Figures from Kalincik et al. “Comparative Effectiveness of Autologous Hematopoietic Stem Cell Transplant vs Fingolimod, Natalizumab, and Ocrelizumab in Highly Active Relapsing-Remitting Multiple Sclerosis”. JAMA Neurology (2023)
Limitations of this study: As reported by the author, ocrelizumab showed similar outcomes as AHSCT in preventing relapses. “While this may be attributed to the shorter study follow-up available in the ocrelizumab cohort, it may also be due to the differences in the mechanisms of action among the therapies.” (Kalincik et al., 2023). Note that the number of patients at risk was very small for both groups. At the end of the follow-up, there were just 1 for AHSCT and 3 for ocrelizumab.
Different types of conditioning regimens were shown, each presenting risks and benefits. It should be noted that the data of this study, are incomplete; for example, data on DMTs pre-AHSCT and pre-comparators, approximately 2 out of 3 patients are missing. MRI data are also missing in this study.
Finally, there is a lack of true randomization.
Table from Kalincik et al. “Comparative Effectiveness of Autologous Hematopoietic Stem Cell Transplant vs Fingolimod, Natalizumab, and Ocrelizumab in Highly Active Relapsing-Remitting Multiple Sclerosis”. JAMA Neurology (2023)
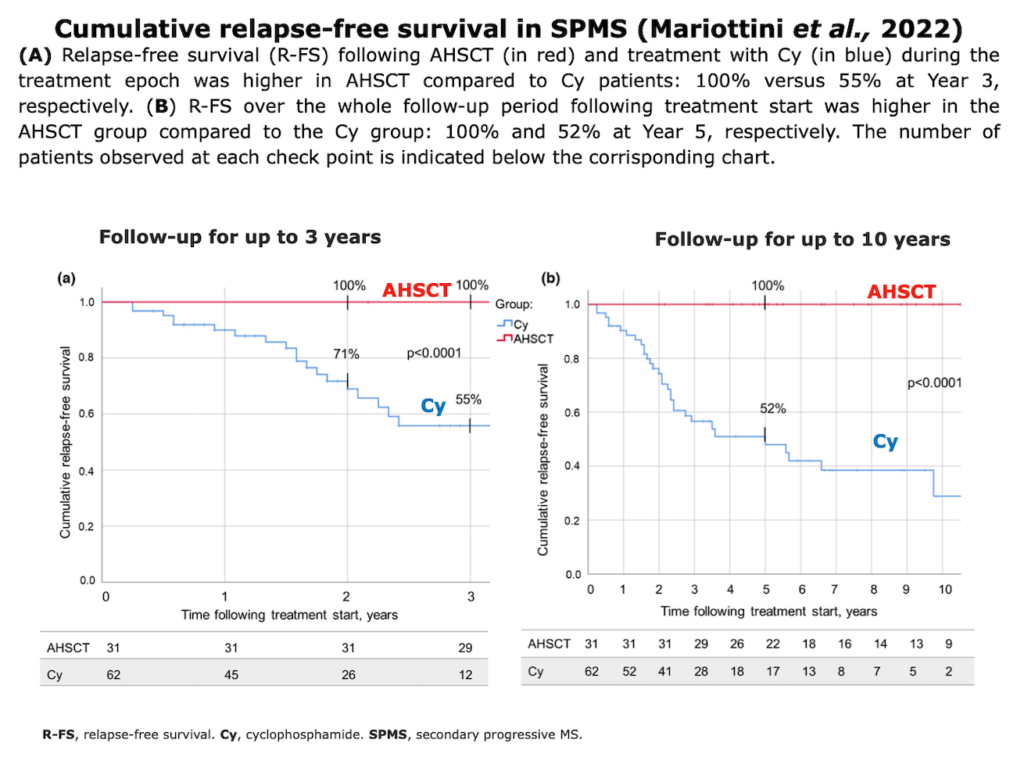
Mariottini et al., 2022. “Autologous haematopoietic stem cell transplantation versus low-dose immunosuppression in secondary–progressive multiple sclerosis”. European Journal of Neurology
The authors compared the effectiveness in 93 patients with SPMS who underwent AHSCT (31 AHSCT-treated patients) vs low-dose immunosuppression with IV cyclophosphamide (Cy) as a comparative treatment (62 Cy-treated patients), using relapses and disability as main outcome measures. Therefore, patients received treatments between 1991 and 2018 at the Careggi University Hospital in Florence (Italy). The study was designed so that for each patient treated with AHSCT, there were two Cy controls (1:2 matched controls). “Controls were selected according to baseline characteristics adopting cardinality matching after trimming on the estimated propensity score” Mariottini et al., 2022.
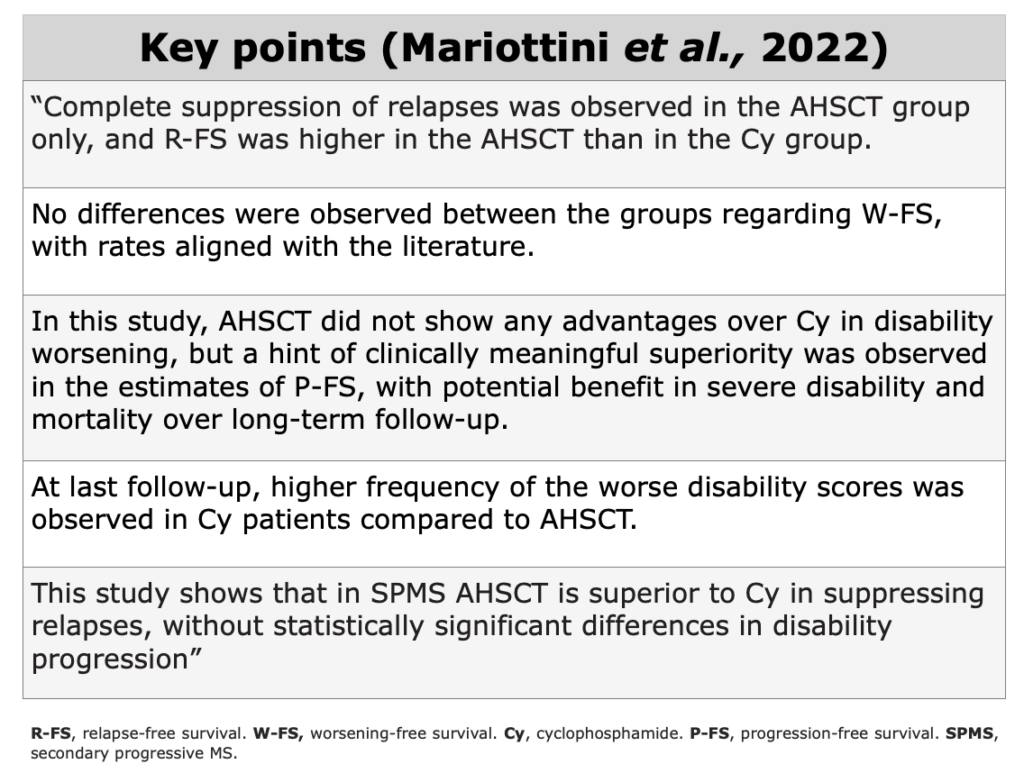
“This study provides Class III evidence, in SP-MS, on the superior effectiveness of AHSCT compared to Cy on relapse activity, without differences on disability accrual. Although the suppression of relapses was observed in the AHSCT group only, AHSCT did not show advantages over Cy on disability, suggesting that in SP-MS disability progression becomes based more on noninflammatory neurodegeneration than on inflammation” (Mariottini et al., 2022).
Mariottini et al. “Autologous haematopoietic stem cell transplantation versus low-dose immunosuppression in secondary–progressive multiple sclerosis”. European Journal of Neurology (2022)
Limitations of this study: “Its observational design does not allow the complete exclusion of residual unknown confounders, and therefore potential inclusion biases might remain unbalanced between the two groups, despite the matching. However, potential confounders had been accurately selected. Moreover, the study was accurately designed, generating a dataset that was matched blind to the outcome variables. In addition, the sensitivity analyses performed confirm the robustness of the results. Given that the covariates that are still unbalanced or are unobserved should plausibly lead to an underestimation of the beneficial effect of AHSCT, the results that were obtained could be considered as a lower bound for the true effect.” (Mariottini et al., 2022).
Case-Series
Patti et al. “Autologous Hematopoietic Stem Cell Transplantation in Multiple Sclerosis Patients: Monocentric Case Series and Systematic Review of the Literature”. Journal of Clinical Medicine
The data was collected from 6 patients who had received transplant between 2019 and 2022 at the Hematology Department at the Hospital “G. Rodolico—San Marco”, University of Catania (Italy). 3 out of 6 patients were female. 3 patients were affected by highly active RRMS, while the others had SPMS. All 6 patients underwent a BEAM+ATG conditioning regimen.
This paper provides an extend review on studies about the use of AHSCT in MS. Read the study here.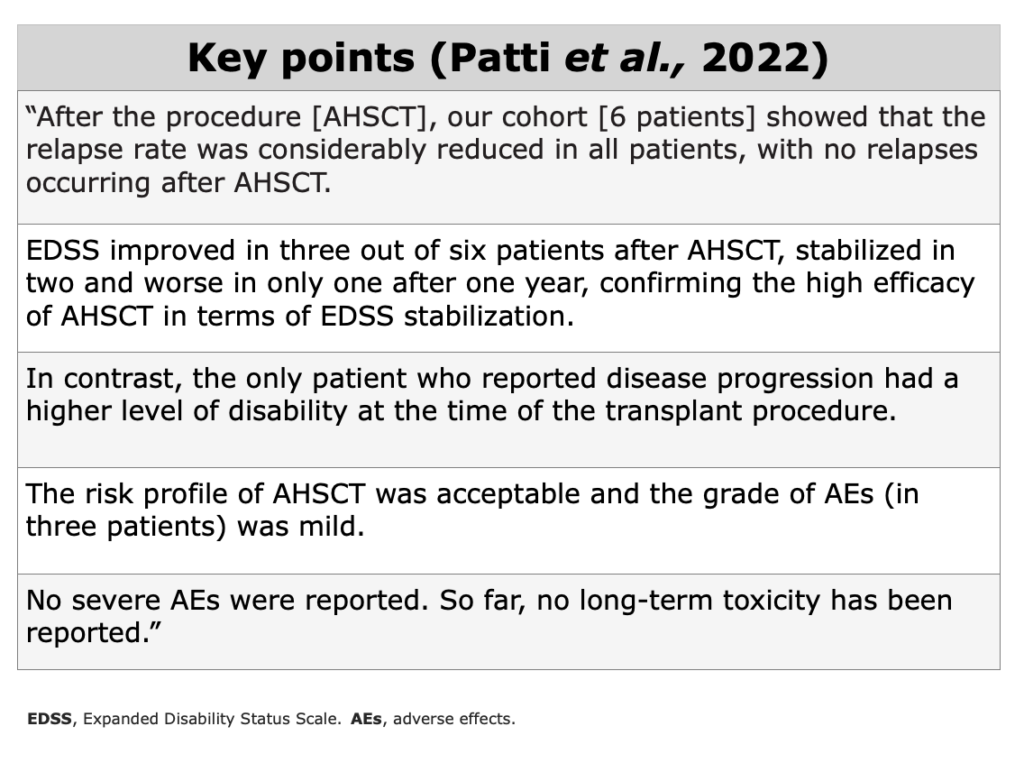
Limitations of this study: limited follow-up (16.6 ± 9.8 months).
Meta-Analysis
While clinical trials produce new experimental evidence, meta-analyses summarize and integrate existing evidence.
Meta-analysis has a qualitative component (i.e., classification of studies according to predetermined characteristics capable of influencing results, such as study design, completeness and quality of data, absence of biases), and a quantitative component (i.e., extraction and analysis of the numerical information).”
Sormani et al., 2017 “Autologous hematopoietic stem cell transplantation in multiple sclerosis. A meta-analysis”. Neurology
This metanalysis reported AHSCT from 1995 to 2016. A total of 15 papers were included, including a total of 764 transplanted patients. 14 out of 15 were open-label uncontrolled studies and 1 was ASTIMS (a randomized study): 5 studies were retrospective, whereas 10 were assessed prospectively. Only one study has compared transplant vs mitoxantrone (ASTIMS trial).
“The emerging evidence on this therapeutic approach AHSCT in MS indicates that the largest benefit/risk profile form this therapeutic approach can be obtained in patients with aggressive MS with a relapsing-remitting course and who have not yet accumulated a high level of disability.” (Sormani et al., 2017).
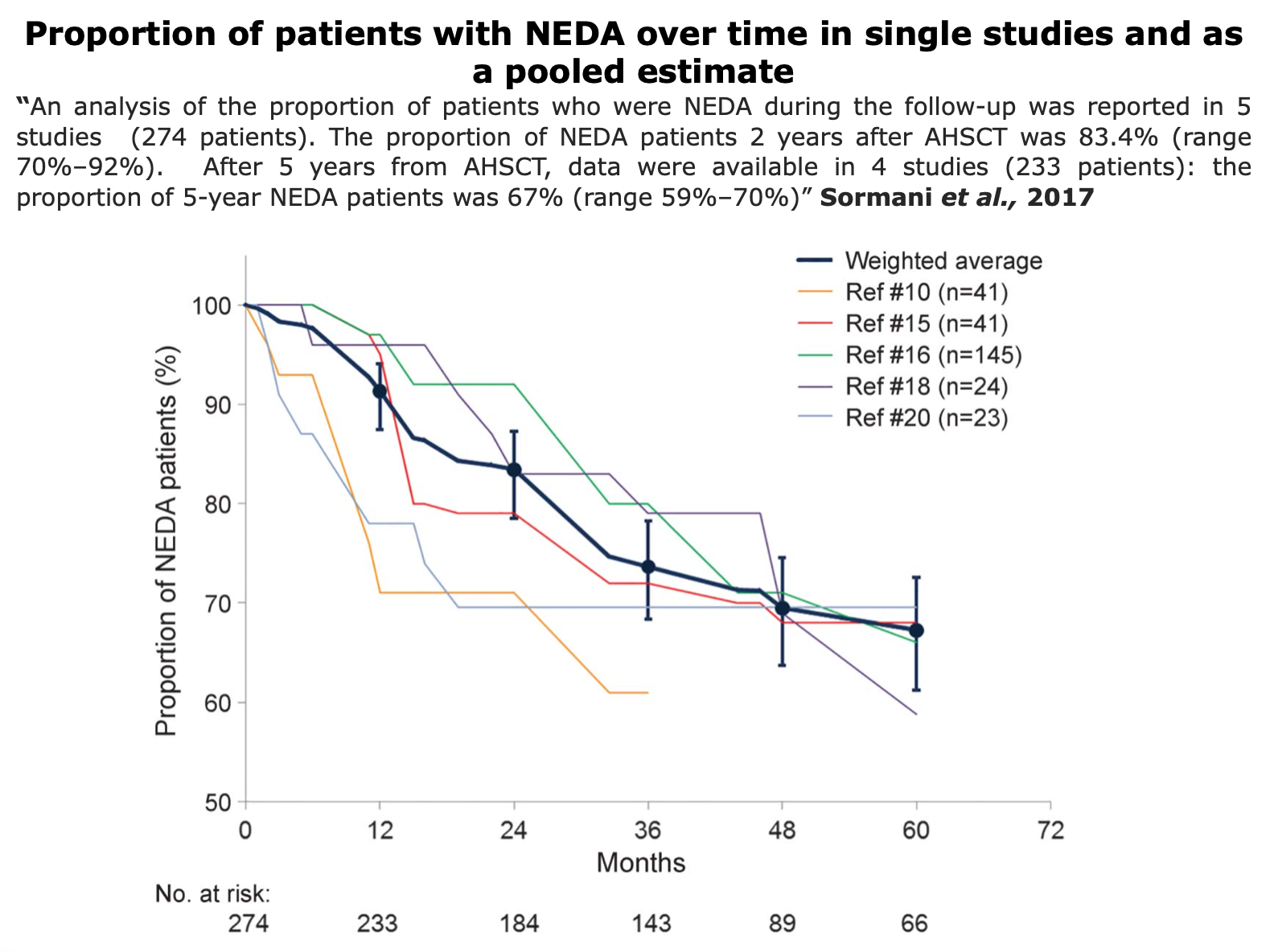
Figure from Sormani et al. “Autologous hematopoietic stem cell transplantation in multiple sclerosis. A meta-analysis”. Neurology (2017)
NOTE THAT: The TRM in this meta-analysis, was 2.1%, which appears particularly high. This is due to the heterogeneity of the sample. This data needs to be interpreted with caution as many studies suggest that the TRM rate in pwMS with RRMS is very close to zero compared to SPMS patients (Sormani et al., 2017). This further underscores the importance of careful patient selection must be done by the transplant center.
The decrease in TRM observed over the years across studies is likely due to improved patient selection, which excludes individuals with advanced disabilities who are at higher risk of complications, and the less frequent use of intensive conditioning regimens in this population.
Limitations: There were some heterogeneities among the studies, in particular regarding the patients’ characteristics, that could introduce some bias. Different conditioning regimens have been used among the studies.
Expert Opinion
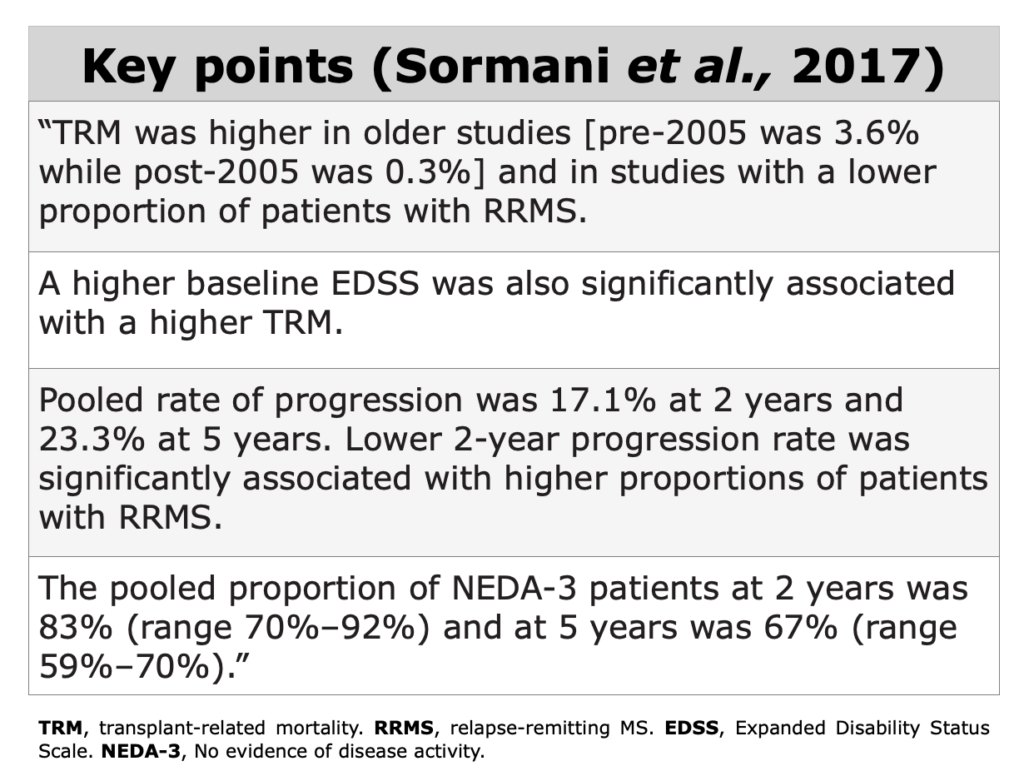
Sormani et al. “NEDA status in highly active MS can be more easily obtained with autologous hematopoietic stem cell transplantation than other drugs”. Multiple Sclerosis Journal
In this paper by Sormani et al., highlighted the relationship in highly active MS and NEDA. “NEDA itself could be an important goal for treating individual patients with RRMS and perhaps even more so as a potential outcome for clinical trials. However, many RRMS patients experience breakthrough disease activity even when receiving the most effective approved DMTs. The proportion of patients achieving the NEDA status under treatment was recently reviewed, ranging from 13% to 46% after 2 years of treatment. Over the long term, the NEDA status is hardly maintained in real-life cohorts.” (Sormani et al., 2017)
The authors note that “immunoablative therapy followed by AHSCT has been investigated for the past two decades to manage severe and treatment-refractory MS. However, the clinical experience indicates this therapy may be way more successful if performed in the early inflammatory stages of MS.”
As reported by the author, the proportion of NEDA patients among those treated with AHSCT is significantly and consistently higher than among those treated with other drugs.
The clinical data, at the time of this paper’s publication, demonstrated that not only did the groups treated with AHSCT achieve higher NEDA rates. This result could therefore be challenged by the heterogeneity of the sample (age, sex, ethnicity), but as the authors argue, the typical profile of a patient undergoing AHSCT is usually that of a patient with an aggressive form of MS. “This makes the higher proportion of NEDA patients achieved with AHSCT as compared to other therapies even more relevant.” Sormani et al., 2017.
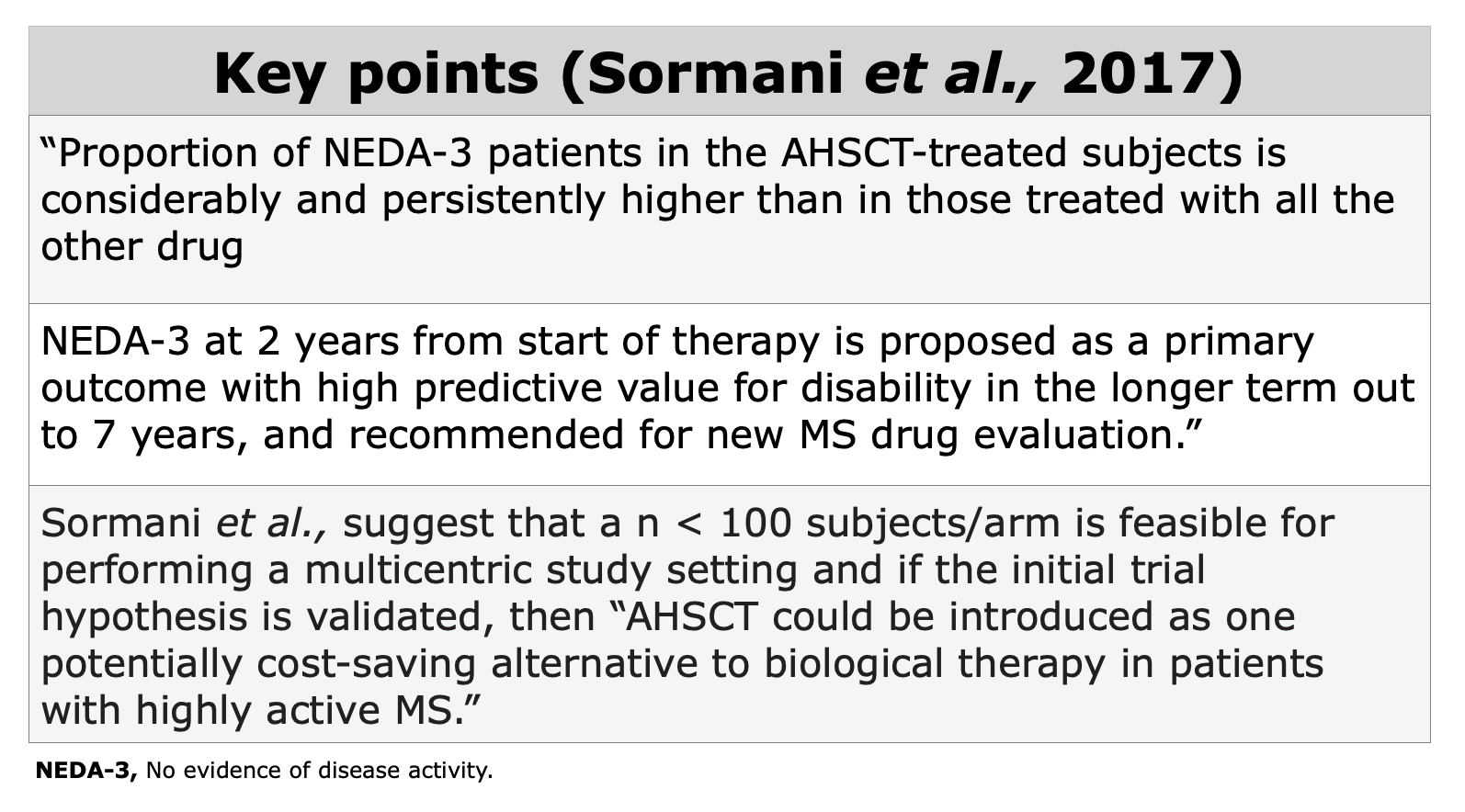
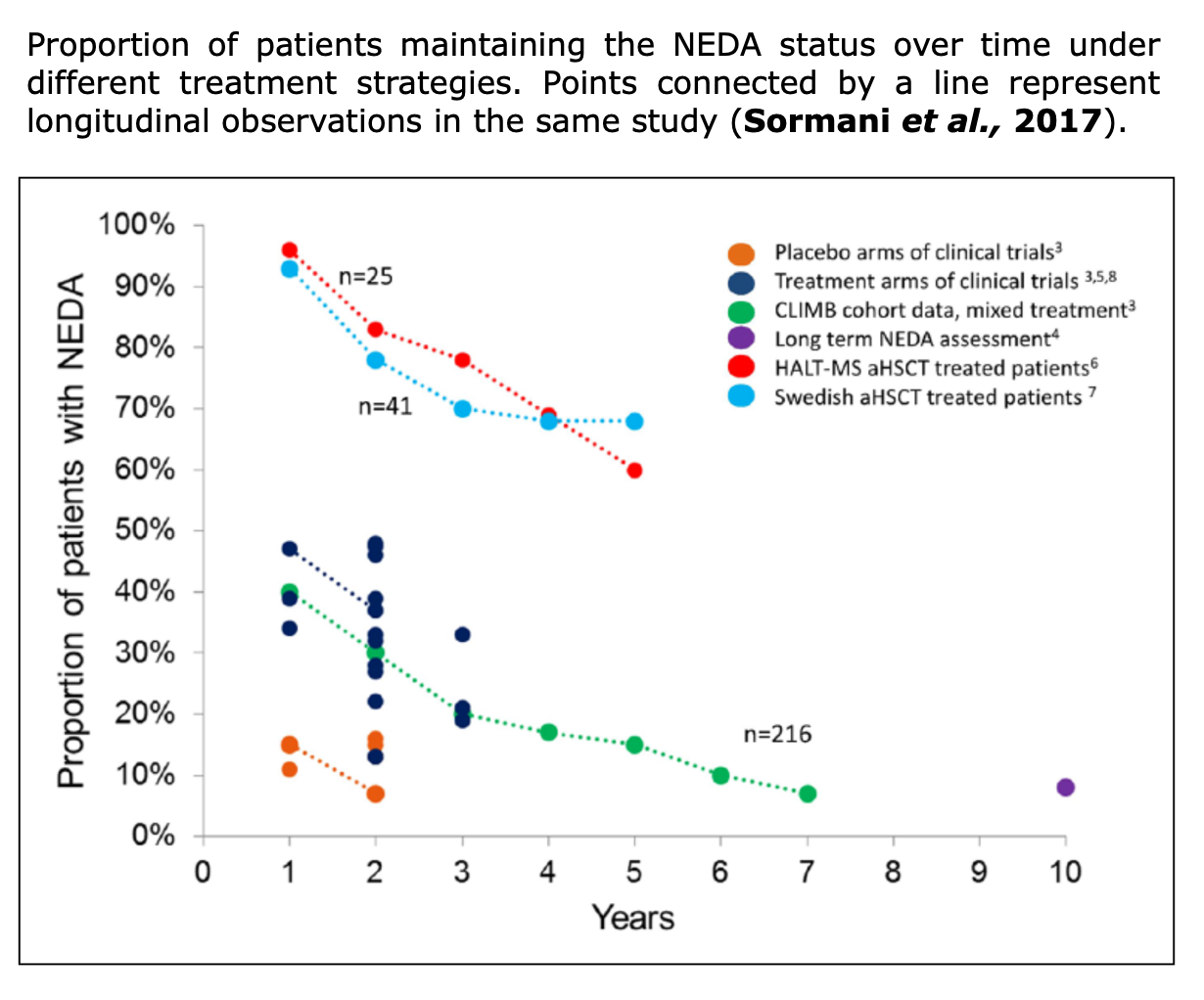
Figure from Sormani et al. “NEDA status in highly active MS can be more easily obtained with autologous hematopoietic stem cell transplantation than other drugs”. Multiple Sclerosis Journal (2017).
Systemic Review
According to “A Dictionary of Epidemiology” (Miguel Porta, 2014), a systemic review “focus on peer-reviewed publications about a specific health problem and use rigorous, standardized methods for selecting and assessing articles. A systematic review differs from a meta-analysis in not including a quantitative summary of the results.”
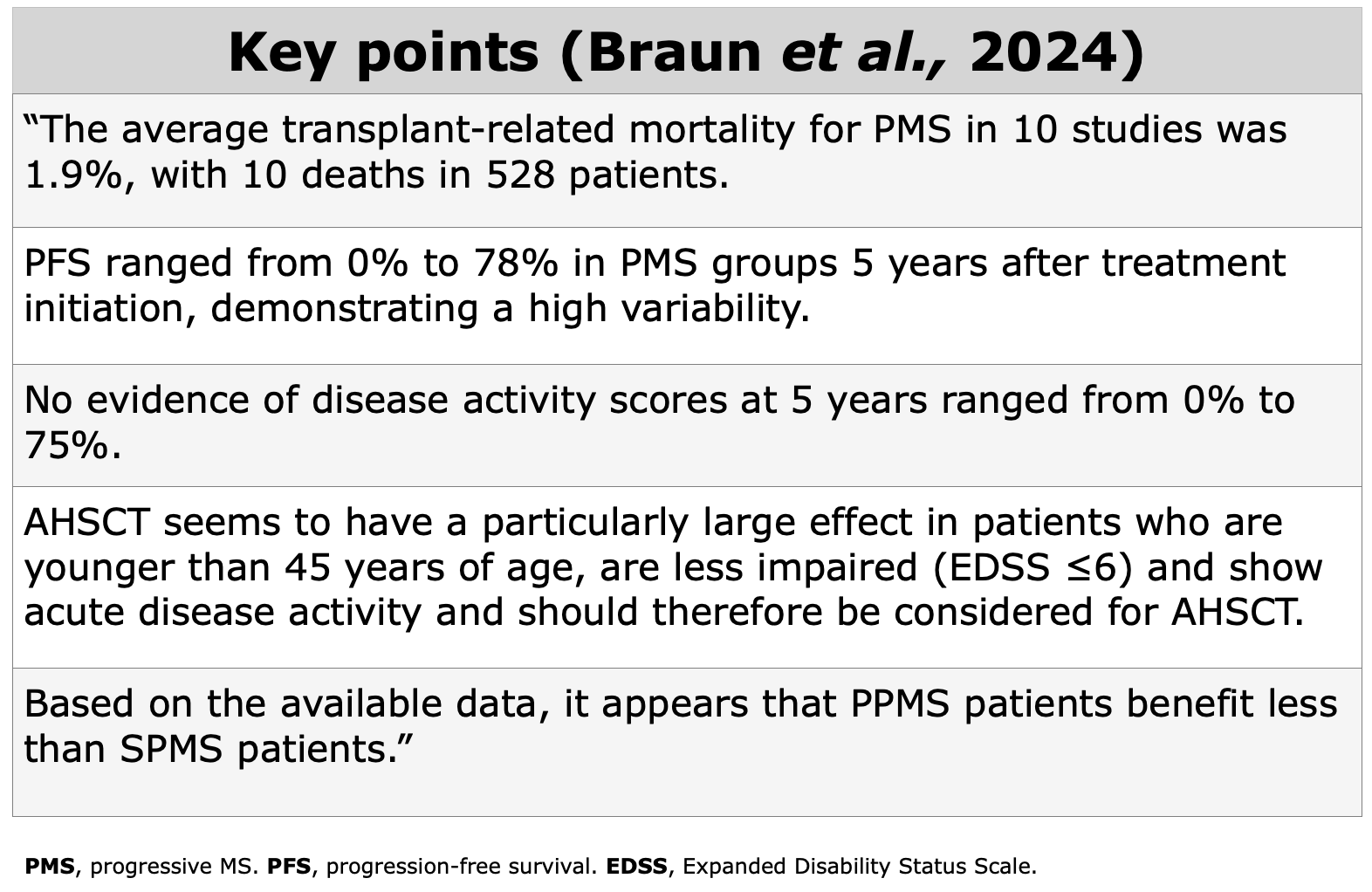
Braun et al. “Exploring the therapeutic potential of autologous hematopoietic stem cell transplantation in progressive multiple sclerosis—a systematic review”. European Journal of Neurology.
This systematic review includes papers on AHSCT published between 2006 and February 2024. A total of 15 studies met the criteria including 665 pwMS with progressive MS (74 PPMS and 591 SPMS), and 801 pwMS with RRMS as controls.
The mean follow-up ranged from 1.6 to 9.6 years. 12 out of 15 studies in this review, reported an EDSS score at baseline of 6.0. The mean disease duration ranged from 2.5 to 13.7 years before AHSCT.
Immunological Evidences
How Does AHSCT Act on the Immune System?
Clinical data suggest that the immune reconstitution (IR) following transplant is associated with sustained therapeutic benefits (read “Clinical evidences” section). The precise mechanisms by which AHSCT provides therapeutic effects remain unclear (Massey et al., 2018), however immunological data indicates that AHSCT in MS involves a reset of the immune system through:
- Ablation (destruction) of pathogenic autoreactive immune cells
- Immune reconstitution from myeloid or lymphoid progenitor cells
- Fast recovery of innate immunity cells (neutrophils, macrophages, and NK cells), which return to baseline levels (few weeks after AHSCT)
- Slow recovery of adaptative immune cells (3-6 months)
- Slower recovery in regulatory cell levels (6-12 months)
- Normalization of immunological functions.
Additional insights can be found in the reviews Arruda et al., 2017, Cencioni et al., 2021 and Mariottini et al., 2023.
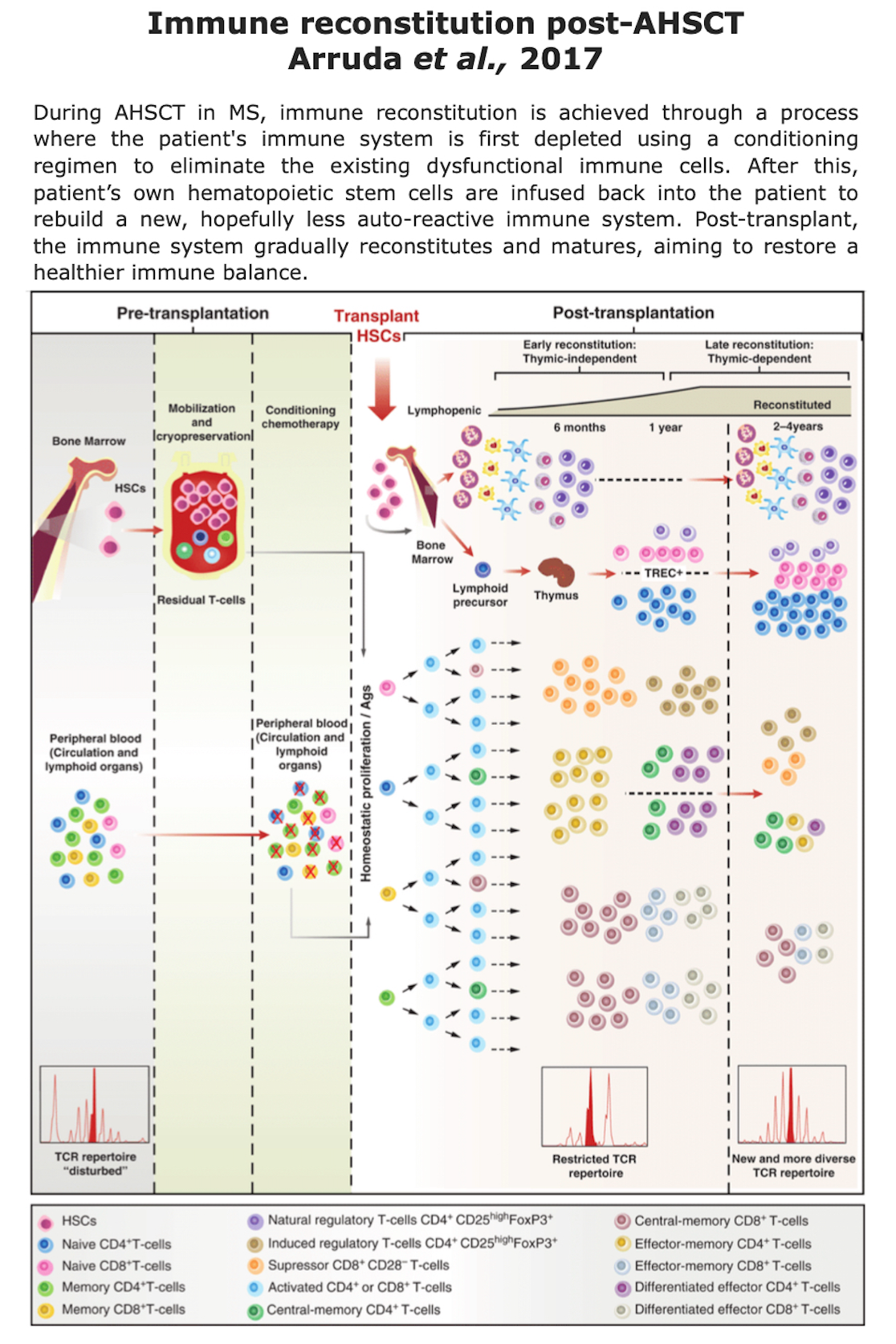
Figure from Arruda et al. “Section 15 Hematopoietic Cell Transplants for Non-Neoplastic Diseases. Autologous Hematopoietic Cell Transplants for Autoimmune Diseases: Specific Diseases and Controversies”. Cambridge University Press (2017).
Papers on Immune Reconstitution Post-AHSCT
Below, some recent papers on the impact on immune reconstitution post-transplant. Click on the authors’ name to read the abstract or the full article where available. This section currently is in progress.
Abstract: “MicroRNAs (miRNAs) are regulators of gene expression and have been reported to be dysregulated in people with multiple sclerosis (pwMS). Autologous hematopoietic stem cell transplantation (aHSCT) is an immune-ablative treatment intervention for pwMS. Currently, it is unknown if aHSCT affects expression levels of miRNAs in CSF (Cerebrospinal fluid). We explored the ability of circulating miRNA to discriminate between pwMS and healthy controls (HCs) and investigated whether these miRNAs were affected by treatment with aHSCT”. (Pavlovic et al., 2024)
Results: “Twelve miRNAs were dysregulated in pwMS compared with HC (q < 0.05). Associations with clinical and analytical parameters were observed in relation to all 12 miRNAs; however, a cluster of 4 miRNAs (miR-16-5p, miR-21-5p, miR-150-5p, and miR-146a-5p) with strong correlations (r > 0.60, p < 0.001) with multiple parameters was identified. Of the 12 miRNAs, 8 were differentially expressed in pwMS with gadolinium-enhancing lesions at baseline and 4 by prior disease-modifying treatment class (p < 0.05). These 4 miRNAs correlated strongly with each other, decreased after aHSCT, and remained low throughout the follow-up period (p < 0.05). Target and pathway analysis of these revealed association with biological processes affecting cytokine production, inflammatory response, and regulation of myelin maintenance.” (Pavlovic et al., 2024)
Discussion: “miRNAs are dysregulated in CSF from pwMS and particularly in patients with less effective treatments and/or higher inflammatory disease activity. A 4-miRNA signature with elevated expression of miR-16-5p, miR-21-5p, miR-150-5p, and miR-146a-5p was recurring in multiple analyses. After intervention with aHSCT, the expression levels approached the levels of the HCs, suggesting a potent treatment effect.” (Pavlovic et al., 2024)
Thymic atrophy typically occurs with age; however, under specific conditions, thymopoiesis can be triggered by infections, burns, surgery, chemotherapy used in the treatment of malignancies, or during AHSCT.
Immune reconstitution following AHSCT occurs in two distinct phases: (1) an early phase, driven primarily by the homeostatic expansion of cells that survive chemotherapy, and (2) a late phase, facilitated by de novo thymopoiesis.
15 patients (7 out of 15 were RRMS), underwent AHSCT at the Cell Therapy and Transfusion Medicine Unit of the Careggi University Hospital in Florence (Italy), in collaboration with the MS Referral Centre for the Tuscany region of the same hospital. All patients received DMTs before AHSCT.
CT scans were performed for clinical purpose, primarily to investigate lung infections in 12 patients (80%). Additionally, (13%) 2 patients underwent total-body CT for EBV-related post-transplant lymphoproliferative disorder (PTLD) staging, and 1 (7%) had pulmonary CT angiography to monitor intracardiac thrombosis prior to AHSCT.
Chest CT scans from these 15 patients were analyzed, with a median of 2 months post-AHSCT. Thymic hyperplasia was observed in 20% of cases (3 out of 15 patients), exclusively in females aged 30–40, within 1–3 months post-AHSCT. According to the Authors, no significant associations with clinical or demographic characteristics, or post-transplant outcomes, were identified.
These findings align with previous research highlighting the role of AHSCT in promoting thymic reactivation and de-novo thymopoiesis, further emphasizing its contribution to immune reconstitution in MS patients.
Marchi et al., 2024 “Leptomeningeal enhancement in multiple sclerosis: a focus on patients treated with hematopoietic stem cell transplantation”. Front. Neurol. Sec. Multiple Sclerosis and Neuroimmunology.
Background: Leptomeningeal enhancement (LME) is “a nonspecific imaging feature present across many neurological disorders, including neoplasm, infection, and primary neuroinflammation. The presence of LME is associated with worse clinical and imaging outcomes in multiple sclerosis, justifying its ascertainment in clinical practice” Ineichen et al., 2021. One goal of therapies is to eliminate them.
This study by Marchi et al. documents that at least in one of the patients with AHSCT, the LME disappeared. This suggests that the chemotherapy used in the transplant (BEAM+ATG) is potentially capable of eliminating one of the localized immunological factors in the CNS.
Aim: LME has been proposed as a potential
Key insights: “the observation of a direct correlation between the number of LMEs and patients” age at AHSCT, but not at MRI, and the disappearance of one LME focus after AHSCT in one case suggest that AHSCT may halt the formation of new LMEs. If this hypothesis was true, early treatment with high-efficacy therapies reaching the CNS compartment could reduce leptomeningeal inflammatory infiltrates organized in ELFs [Ectopic Lymphoid Follicle-like structures] and possibly prevent (or revert) the compartmentalization of inflammation. Longitudinal prospective studies with long-term follow-up are needed to clarify if LME can represent a marker of response to treatments bioavailable within the CNS.” Marchi et al., 2024
Conclusions: “disappearance of one LME focus after AHSCT in one case suggest that AHSCT may halt the formation of new LMEs.” Marchi et al., 2024. Initiating treatment early with high-efficacy therapies that penetrate the CNS compartment could reduce leptomeningeal inflammatory infiltrates organized in ELFs and potentially prevent or reverse the compartmentalization of inflammation.
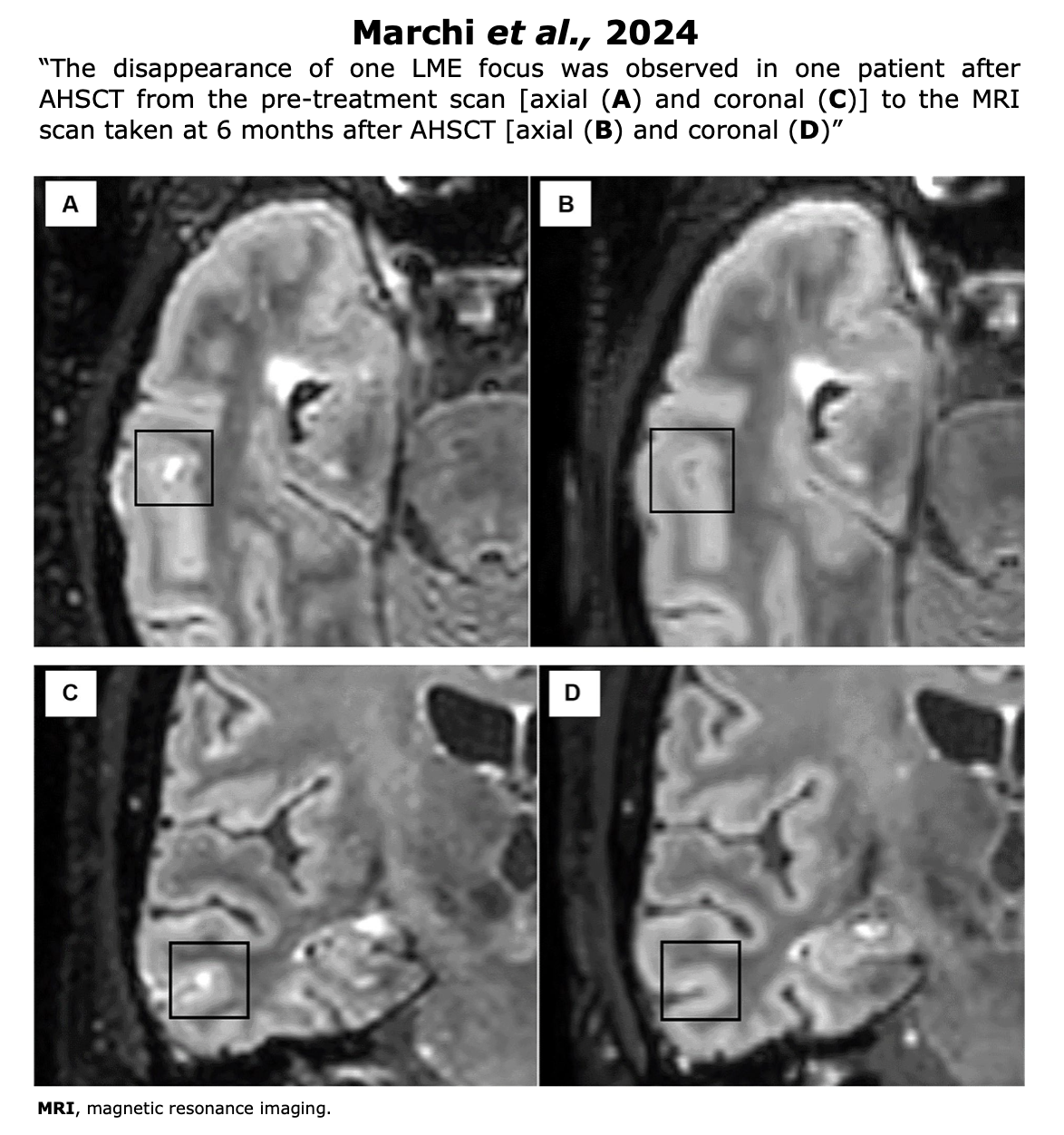
Figure from Marchi et al. “Leptomeningeal enhancement in multiple sclerosis: a focus on patients treated with hematopoietic stem cell transplantation”. (2024) Front. Neurol. Sec. Multiple Sclerosis and Neuroimmunology.
Ruder et al., 2022 “Dynamics of T cell repertoire renewal following autologous hematopoietic stem cell transplantation in multiple sclerosis”. Science Translational Medicine.
Abstract: “Autologous hematopoietic stem cell transplantation (AHSCT) is a highly effective treatment of MS. It depletes autoreactive cells and subsequently renews adaptive immune cells. The possible proinflammatory potential of surviving T cells early after AHSCT has not been studied.
Here, we examined the dynamics of new and surviving T cells in 27 patients after AHSCT by multidimensional flow cytometry, T cell receptor (TCR) sequencing, specificity testing, telomere length profiling, and HLA genotyping. Early after AHSCT, naïve T cells are barely detectable, whereas effector memory (EM) T cells quickly reconstitute to pre-AHSCT values. EM CD4+ T cells early after AHSCT have shorter telomeres, have higher expression of senescence and exhaustion markers, and proliferate less than those before AHSCT.
We find a median TCR repertoire overlap of 26% between the early post-AHSCT EM CD4+ T cells and pre-AHSCT, indicating persistence of EM CD4+ T cells early after transplantation. The EM CD4+ TCR repertoire overlap declines to 15% at 12 months after AHSCT, whereas the naïve TCR repertoire entirely renews. HLA-DR–associated EM CD4+ T cell reactivity toward MS-related antigens decreased after AHSCT, whereas reactivity toward EBV increased.
Our data show substantial survival of pre-AHSCT EM CD4+ T cells early after transplantation but complete renewal of the T cell repertoire by nascent T cells later.”
von Niederhäusern et al., 2022 “B-Cell Reconstitution After Autologous Hematopoietic Stem Cell Transplantation in Multiple Sclerosis”. Neurology Neuroimmunol Neuroinflamm
Abstract: “Total B-cell numbers recovered within 3 months and increased above normal levels 1 year after transplantation, successively shifting from a predominantly transitional to a naive immune phenotype. Memory subpopulations recovered slowly and remained below normal levels with reduced repertoire diversity 1 year after transplantation.
Isotype subclass analysis revealed a proportional shift toward IgG1-expressing cells and a reduction in IgG2 cells. Mutation analysis of IgH sequences showed that highly mutated memory B cells and plasma cells may transiently survive conditioning while the analysis of sequence cluster overlap, variable (IGHV) and joining (IGHJ) gene usage and repertoire diversity suggested a renewal of the late post-transplant repertoire. In patients with early cytomegalovirus reactivation, reconstitution of naive and memory B cells was delayed. Our detailed characterization of B-cell reconstitution after AHSCT in MS indicates a reduced reactivation potential of memory B cells up to 1 year after transplantation, which may leave patients susceptible to infection, but may also be an important aspect of its mechanism of action”
Abstract: “MS is an autoimmune disease of the central nervous system, in which autoreactive T and B cells play important roles. Other lymphocytes such as NK cells and innate-like T cells appear to be involved as well. To name a few examples, CD56bright NK cells were described as an immunoregulatory NK cell subset in MS while innate-like T cells in MS were described in brain lesions and with proinflammatory signatures. Autologous hematopoietic stem cell transplantation (AHSCT) is a procedure used to treat MS. This procedure includes hematopoietic stem/progenitor cell (HSPC) mobilization, then high-dose chemotherapy combined with anti-thymocyte globulin (ATG) and subsequent infusion of the patients own HSPCs to reconstitute a functional immune system. AHSCT inhibits MS disease activity very effectively and for long time, presumably due to elimination of autoreactive T cells. Here, we performed multidimensional flow cytometry experiments in peripheral blood lymphocytes of 27 MS patients before and after AHSCT to address its potential influence on NK and innate-like T cells. After AHSCT, the relative frequency and absolute numbers of CD56bright NK cells rise above pre-AHSCT levels while all studied innate-like T cell populations decrease. Hence, our data support an enhanced immune regulation by CD56bright NK cells and the efficient reduction of proinflammatory innate-like T cells by AHSCT in MS. These observations contribute to our current understanding of the immunological effects of AHSCT in MS.”
Cencioni et al., 2021 “Immune Reconstitution Following Autologous Hematopoietic Stem Cell Transplantation for Multiple Sclerosis: A Review on Behalf of the EBMT Autoimmune Diseases Working Party”. Front Immunol
Abstract: “Multiple sclerosis (MS) is a central nervous system (CNS) disorder, which is mediated by an abnormal immune response coordinated by T and B cells resulting in areas of inflammation, demyelination, and axonal loss. Disease-modifying treatments (DMTs) are available to dampen the inflammatory aggression but are ineffective in many patients. Autologous hematopoietic stem cell transplantation (HSCT) has been used as treatment in patients with a highly active disease, achieving a long-term clinical remission in most.
The rationale of the intervention is to eradicate inflammatory autoreactive cells with lympho-ablative regimens and restore immune tolerance. Immunological studies have demonstrated that autologous HSCT induces a renewal of TCR repertoires, resurgence of immune regulatory cells, and depletion of proinflammatory T cell subsets, suggesting a “resetting” of immunological memory. Although our understanding of the clinical and immunological effects of autologous HSCT has progressed, further work is required to characterize the mechanisms that underlie treatment efficacy.
Considering that memory B cells are disease-promoting and stem-like T cells are multipotent progenitors involved in self-regeneration of central and effector memory cells, investigating the reconstitution of B cell compartment and stem and effector subsets of immunological memory following autologous HSCT could elucidate those mechanisms. Since all subjects need to be optimally protected from vaccine-preventable diseases (including COVID-19), there is a need to ensure that vaccination in subjects undergoing HSCT is effective and safe.
Additionally, the study of vaccination in HSCT-treated subjects as a means of evaluating immune responses could further distinguish broad immunosuppression from immune resetting.”
Massey et al., 2018 “Regenerating immunotolerance in Multiple Sclerosis with Autologous Hematopoietic Stem Cell Transplant”. Front Immunol
Abstract: “MS is an inflammatory disorder of the central nervous system where evidence implicates an aberrant adaptive immune response in the accrual of neurological disability. The inflammatory phase of the disease responds to immunomodulation to varying degrees of efficacy; however, no therapy has been proven to arrest progression of disability. Recently, more intensive therapies, including immunoablation with AHSCT, have been offered as a treatment option to retard inflammatory disease, prior to patients becoming irreversibly disabled. Empirical clinical observations support the notion that the immune reconstitution (IR) that occurs following AHSCT is associated with a sustained therapeutic benefit; however, neither the pathogenesis of MS nor the mechanism by which AHSCT results in a therapeutic benefit has been clearly delineated.
Although the antigenic target of the aberrant immune response in MS is not defined, accumulated data suggest that IR following AHSCT results in an immunotolerant state through deletion of pathogenic clones by a combination of direct ablation and induction of a lymphopenic state driving replicative senescence and clonal attrition. Restoration of immunoregulation is evidenced by changes in regulatory T cell populations following AHSCT and normalization of genetic signatures of immune homeostasis. Furthermore, some evidence exists that AHSCT may induce a rebooting of thymic function and regeneration of a diversified naïve T cell repertoire equipped to appropriately modulate the immune system in response to future antigenic challenge. In this review, we discuss the immunological mechanisms of IR therapies, focusing on AHSCT, as a means of recalibrating the dysfunctional immune response observed in MS.”
Burt et al. “New autoimmune diseases after autologous hematopoietic stem cell transplantation for multiple sclerosis”. Bone Marrow Transplantation
A part of this paper is dedicated to IR.
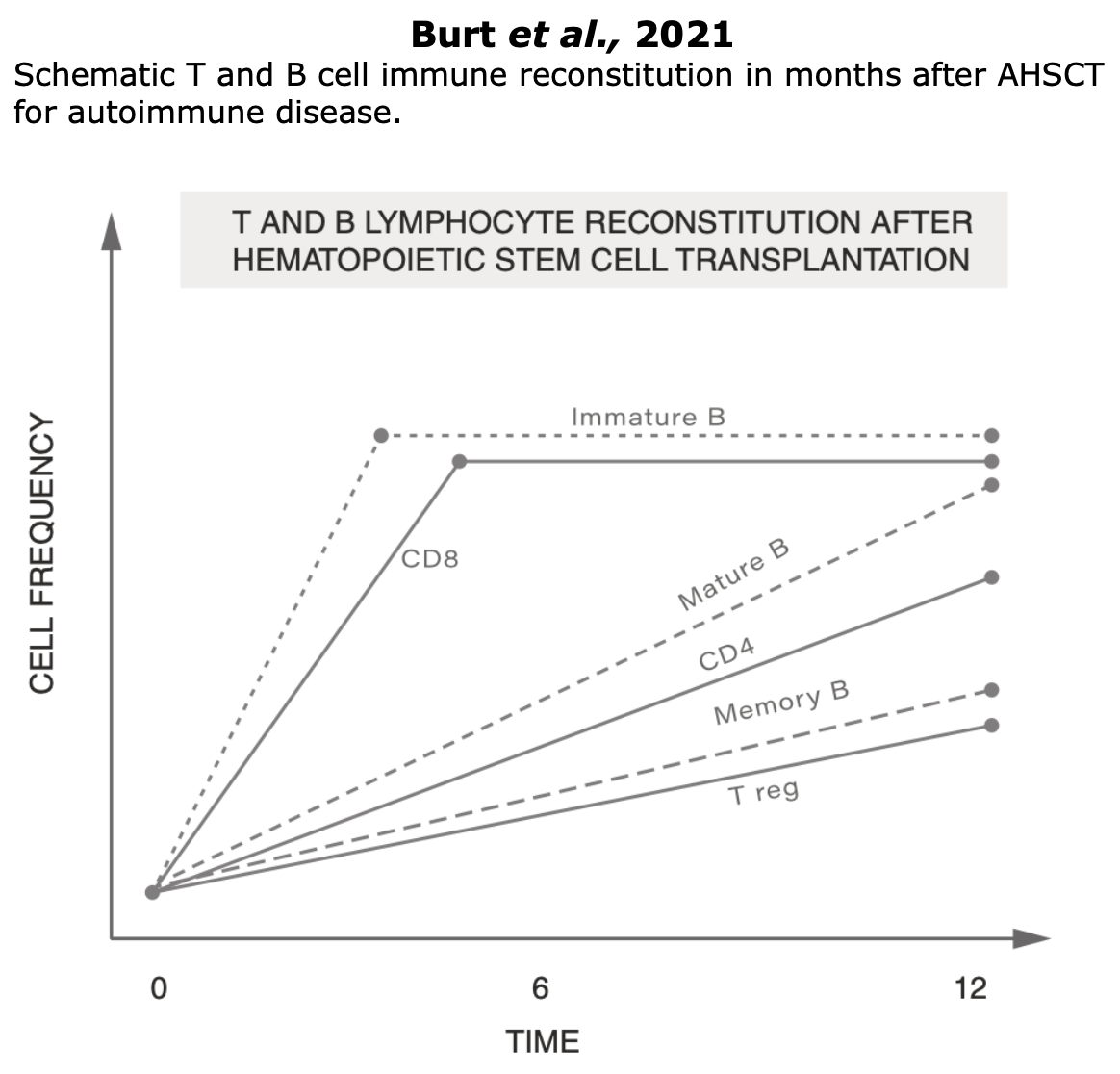
Figure Burt et al.“New autoimmune diseases after autologous hematopoietic stem cell transplantation for multiple sclerosis”. Bone Marrow Transplantation
Quality Of Life
WHO defines Quality of Life (QoL) as “an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns”.
Improvements in health-related QoL have consistently correlated with sustained clinical stabilization (Muraro et al., 2025) and represent the most meaningful outcome for patients, as they directly impact their daily lives.
In pwMS, QoL is affected in numerous ways and aspects, including their ability to work, perform daily activities, and execute everyday tasks (Rezapour et al., 2017).
Initially, only the physical disability caused due to MS was considered by clinicians, as the sole aspect of the disease. In order to obtain an overview on how MS impairs patients’ QoL both psychological aspects and physical aspects must be considered.
All three of the studies listed below, published between 2022-2025, and focused on QoL following AHSCT, have demonstrated a sustained improvement in QoL.
QoL according to FDA: a patient-report outcome
QoL can be considered as a patient-reported outcome (PRO). PROs are defined by the US FDA as the “measurement of any aspect of a patient’s health status that comes directly from the patient, without the interpretation of the patient’s response by a clinician or anyone else” (US Food and Drug Administration 2009) (EBMT handbook – Barata et al., 2024). Consequently, PROs describe the impact that AHSCT has on patients’ lives.
As reported in the EBMT handbook (2024) there are numerous measures for assessing QoL. These measures include both general and disease-specific assessments. Trials like STAR-MS, RAM-MS and NET-MS have included QoL as a secondary outcome, emphasizing that incorporating QoL alongside other measures in clinical and research settings offers a more comprehensive understanding of AHSCT outcomes.
Pharmacoeconomics
Pharmacoeconomics is a specialized branch of economics that assesses the cost and value of pharmaceutical products and services. It examines their cost and the benefits they provide in terms of reducing disease progression, disability, and improving patients’ quality of life (QoL).
Pharmacoeconomics employs various methods, such as cost-effectiveness analysis, to evaluate these aspects. These studies are essential for all healthcare systems, given the increasing challenges in providing medications to all citizens.
Pharmacoeconomic studies has consistently shown that transplants offer greater benefits to patients at a lower cost (“more effective, less costly“) than traditional DMTs. These findings apply to both public healthcare systems (such as in Italy, Norway, and Poland) and private ones.
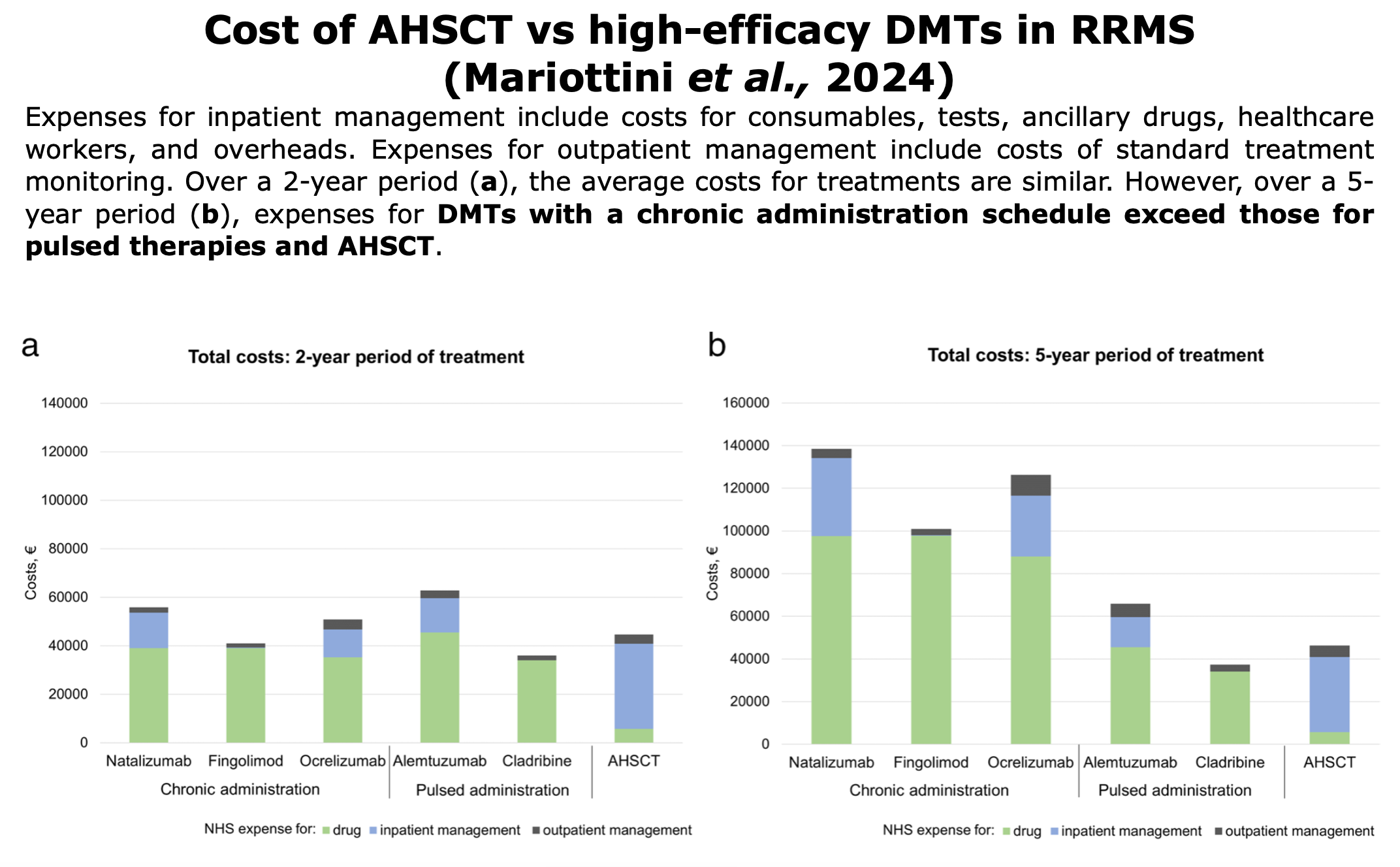
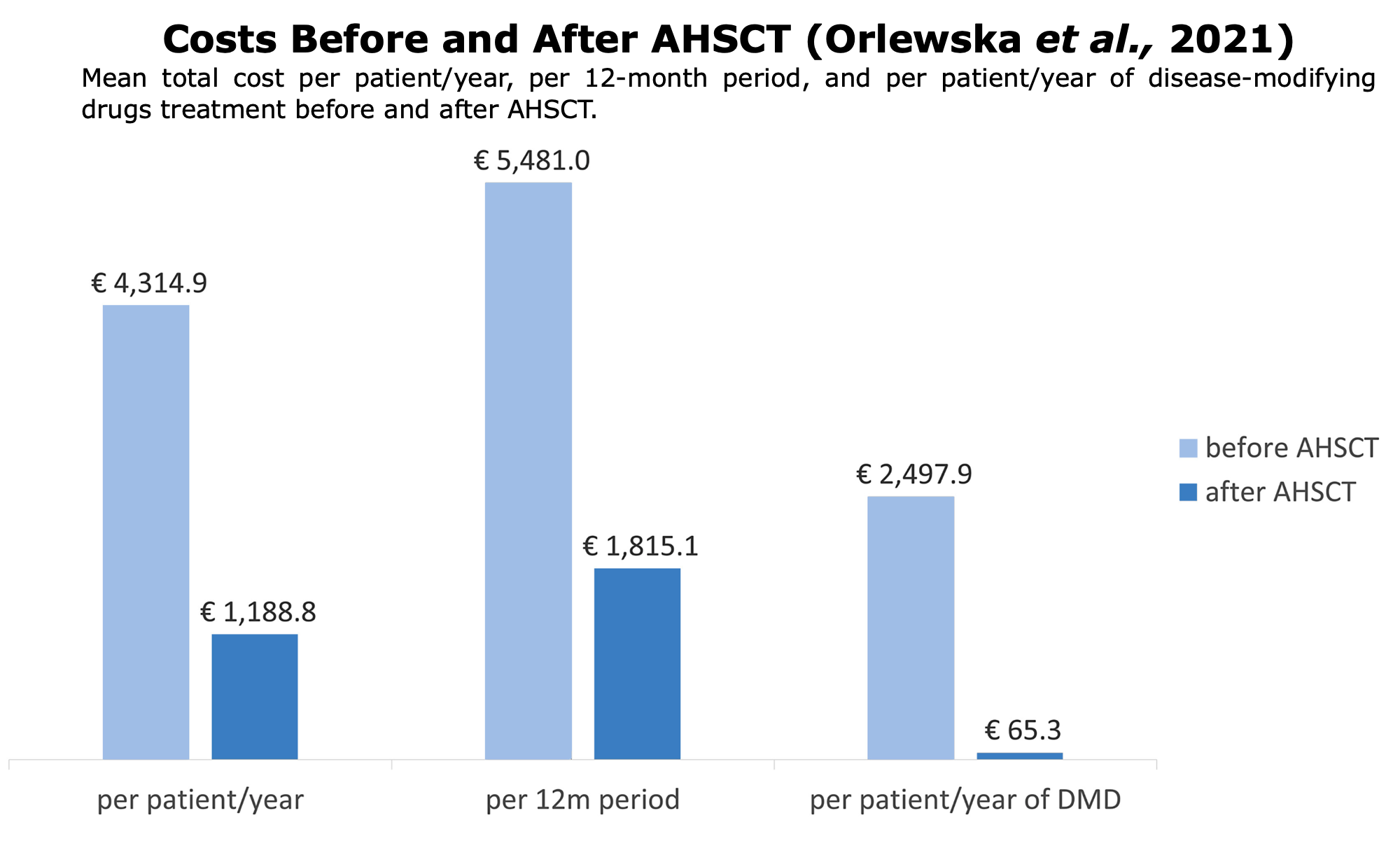
Following studies or reports on pharmacoeconomic around the world comparing AHSCT vs. DMTs: